Previous Issues Volume 4, Issue 1 - 2019
Van Neck-Odelberg Disease
Andrea Nos Colom1*, Jesus Lucas Garcia1, Miguel Angel Edo Prades2, Vicente Olaya Alamar1
1Department of Pediatrics, University General Hospital of Castellon, Spain 2Department of Radiology, University General Hospital of Castellon, Spain
Received Date: Jul 10, 2019 Published Date: Jul 31, 2019
Corresponding Author: Andrea Nos Colom* Pediatric Suite, Pediatric Services, University GeneralHospital of Castellon, Department of Medicine, Cardenal Herrera University-CEU, Valencia, Spain.
Copyright © 2019 Colom AN.
Citation: Colom AN. (2019). Van Neck-Odelberg Disease. Mathews J Pediatr. 4(1): 18. 1
INTRODUCTION
The synchondrosis ischiopubic (SIP) is the cartilaginous union between the lower ischium and pubis branch in infancy. It is a temporary joint which is slimming to obliterate a bone fusion with skeletal maturation. This process, which is completed before puberty, is asymptomatic, however some children develop osteochondritis with pain and lameness.
We describe a 9-year-old girl who had pain in the left inguinal region of 5 days of evolution. Not a traumatic history. Afebrile. Scan it emphasized limitation to the expansion and external rotation of the hip without inflammatory signs. The complete blood count, biochemistry, blood and acute phase reactants were normal. Pelvis AP x-ray (Figure 1) showed widening radiolucent in left SIP associated with irregular margins.
 Figure 1: RX pelvis (anteroposterior). Radiolucid widening of left ischial synchondrosis associated with irregularity of its margins.
Figure 1: RX pelvis (anteroposterior). Radiolucid widening of left ischial synchondrosis associated with irregularity of its margins.
Given the pseudotumoral aspect was carried out magnetic resonance imaging (MRI) for the differential diagnosis with stress fractures, osteomyelitis and tumors. Axial image (proton density) PD (Figure 2) confirms widening of the SIP, as well as the irregularity of the same margins. In the STIR (short tau investment recovery) axial image (Figure 3), the left SIP presents a discrete hyperintensity inside, keeping a hypointense central band, and an edemain the corresponding adjacent bone marrow. This sequence overrides the signal intensity of bone marrow fat allowing you to more easily distinguish the bone edema.
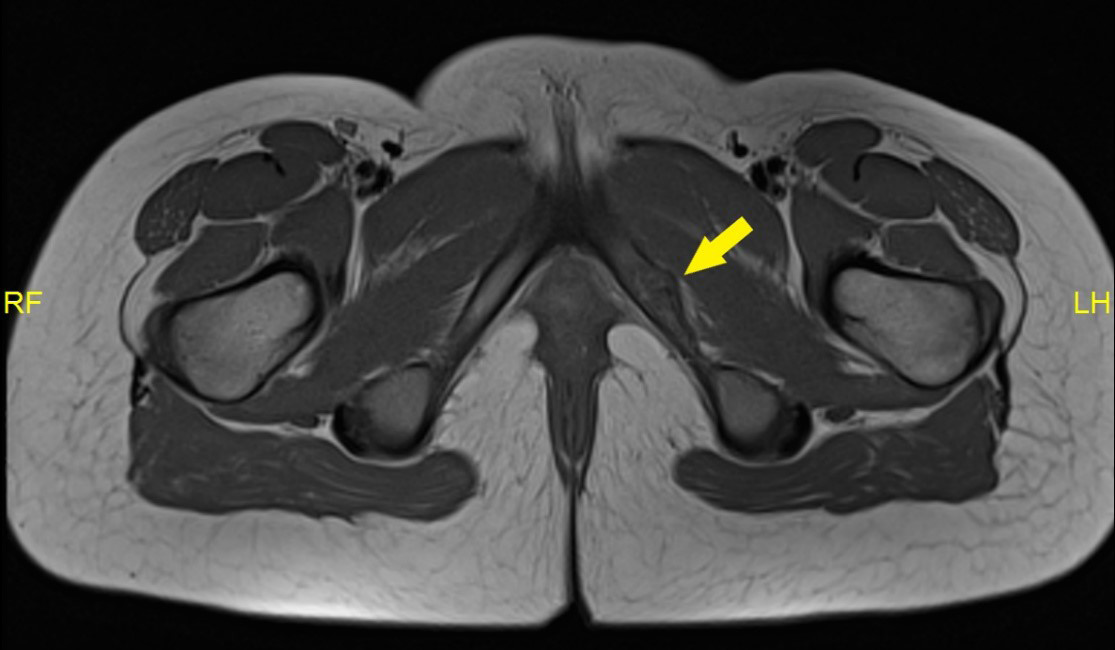 Figure 2: RMN axial pelvis DP (protonic density). Widening ischiopubic synchondrosis, as well as the irregularity of ischiopubic synchondrosis, without associated soft parts component.
Figure 2: RMN axial pelvis DP (protonic density). Widening ischiopubic synchondrosis, as well as the irregularity of ischiopubic synchondrosis, without associated soft parts component.

Figure 3: RMN axial pelvis STIR (short tau investment recovery). Left ischiopubic synchondrosis presents a discrete hyperintensity inside, maintaining a central hypointense band, and in the corresponding adjacent bone marrow with edema. These images confirmed the suspected diagnosis of “Osteochondritis of Van Neck-Odelberg”, prescribing complete rest and anti-inflammatory drugs, with favorable evolution.
REFERENCES
1. Schvartzman P, Varela A, Alarcon V, Salgado D, et al. (2015). Ischiopubic synchondrosis syndrome. Van Neck-Odelberg disease. Rev Argent Radiol. 79: 110-112. 2. Morante I, Ortega M, Clemente D and Lopez J. (2017). Van Neck-Odelberg disease: one more cause of lameness in childhood. Rheumatol Clin. 13 (5): 299-300.