Previous Issues Volume 1, Issue 1 - 2017
The Cytomorphological Spectrum of Papillary Lesions in the Breast
Torill Sauer1 *
Department of Pathology, Akershus University Hospital and University of Oslo, Faculty of Medicine, Institute of Clinical Medicine, Campus Ahus 1478 Lørenskog, Norway. Corresponding Author: Torill Sauer, Department of Pathology, Akershus University Hospital, 1478 Lørenskog, Norway, Tel: +4767964599, E-Mail: [email protected]
Received Date: 20 Sep 2017 Accepted Date: 09 Oct 2017 Published Date: 13 Oct 2017
Copyright © 2017 Sauer T
Citation: Sauer T. (2017). The Cytomorphological Spectrum of Papillary Lesions in the Breast.Mathews J Cytol Histol. 1(1): 005.
ABSTRACT
The objective of this review is to illustrate the broad spectrum of papillary lesions that can be found in breast fine needle aspirations (FNAC). Papillary tumors of the breast comprise lesions of variable morphology and include entities ranging from benign to high grade malignant. Features of papillary neoplasms invariably describe branching three-dimensional papillary clusters with delicate fibrovascular cords. Cytomorphological criteria for benign and low-grade malignant entities overlap and a definite cytological diagnosis is not always possible. Cellular papillomas may harbor areas of ductal carcinoma in situ (DCIS), atypical ductal hyperplasia (ADH) or lobular neoplasia. DCIS can be both high grade and non-high grade. Immunocytochemistry (ICC) can be helpful, providing there is adequate material for ICC. Relatively high error rates, false negatives as well as false positive diagnoses can be found. In general, papillary lesions may be recognized as such. Reporting strategies will often recommend caution if trying to differentiate benign, cellular papillomas from low-grade carcinomas. In conclusion, papillary lesions present with a broad spectrum of cytomorphological features that are illustrated in this review
KEYWORDS
Breast Cytopathology; Cytomorphology; Fine Needle Aspiration; FNB – Proliferative Lesions; Morphology; Papillary Carcinoma.
INTRODUCTION
Papillary tumors of the breast comprise lesions of variable morphology and include entities ranging from benign to high grade malignant (table 1). A papillary neoplasm is histologically one that exhibits an arborescent epithelial proliferation with fibrovascular cores and is attached by a stalk to the wall of a dilated duct. They constitute < 2 % of all breast lesions.
Table 1: Papillary lesions of the breast.
- Intraductal papilloma
- Intraductal papilloma NOS (not otherwise specified) with or without benign hyperplasia
- Intraductal papilloma with atypical ductal hyperplasia
- Intraductal papilloma with lobular neoplasia
- (florid) (subareolar) papillomatosis of the nipple
- Intraductal papillary carcinoma in situ
- Encapsulated papillary carcinoma
- Solid, papillary carcinoma
- Invasive papillary carcinoma
- Invasive micropapillary carcinoma
Cytomorphological criteria for benign and low-grade malignant entities overlap and a definite cytological diagnosis is not always possible. Features of papillary neoplasms invariably describe branching three-dimensional papillary clusters with delicate fibrovascular cords [1-6]. Additional features of papillary carcinomas include moderate to abundant cellular material [2-4], small papillae arranged in cell balls, tall columnar cells, isolated naked nuclei and hemosiderin laden macrophages [2, 3], irregular groups of predominantly monolayered (two-dimensional) epithelium composed of small, polygonal or cuboidal cells with eosinophilic cytoplasm and rounded, eccentrically placed nuclei [2, 3, 7-19]. Features indicating a benign papillary lesion include less cell material, papillae with cohesive stalks surrounded by columnar cells in a honeycomb pattern, apocrine metaplasia, bipolar naked nuclei as well as fewer small papillae and isolated columnar cells [2, 3]. Myoepithelial cells within clusters and inconspicuous naked, bipolar nuclei in the background also indicate a benign lesion [2, 5]. Tse et al report considerable overlaps in the criteria [19] and no demonstrable quantitative differences between papilloma and papillary carcinoma (PC), but with a qualitatively higher degree of atypia in PC and more elaborate and slender papillary fragments. Haji et al found loose cohesive clusters and acinar formation of neoplastic cells to be significant parameters differentiating PC from benign papillomas [20]. Reported accuracy rates in the literature are given as 27 % - 88 % for all papillary lesions [10, 19, 21, 22] and 91 % for PC alone [18]. Prathiba et al and Jayaram et al reported a sensitivity of 42% and 73%, respectively [10, 15] and a specificity of 88.3 % [23]. Relatively high error rates, false negatives (FN) as well as false positive (FP) diagnoses are reported [11, 15, 18, 19]. Not all lesions diagnosed as papillary on cytology are papillary on histology, the most common error being fibroadenomas and fibrocystic changes (10, 18, 21, 24) but in general, papillary lesions can be diagnosed as such [2, 6, 7, 10, 12, 21]. The known and reported criteria of papillary lesions are almost exclusively based on conventional smears. Many institutions now use liquid based preparations (LBC) alone or as an adjunct to traditional smears. Several features may change and appear different in LBC and could potentially cause both
FN and FP diagnoses [24].
The aim of this review is to illustrate the broad spectrum of papillary lesions that can be found in breast FNAC.
Table 2: Cytological findings in (benign) intraductal papillomas.
- Variable cellularity with a basic benign pattern
- Epithelial components:
- Cohesive papillary clusters
- (Micro-) papillary clusters, bipolar cells
- Complex, folded, monolayer or three dimensional epithelial aggregates
- Small groups and monolayer sheets
- Benign nuclei or nuclei showing moderate to distinct cellular/nuclear pleomorphism but with a fine chromatin pattern
- Nucleoli may be distinct
- Hyperplasia with and without atypia showing a mixed cell population, both benign and irregular/atypical with threedimensional aggregates that may resemble ADH/low grade DCIS (solid and/or cribriform)
- Usually the epithelial fragments are rather cohesive
- A (usually small) population of single cells is not uncommon
- Myoepithelial cells/nuclei
- Apocrine cells
- Stromal fragments, partly papillary with vascular core
- Debris and macrophages
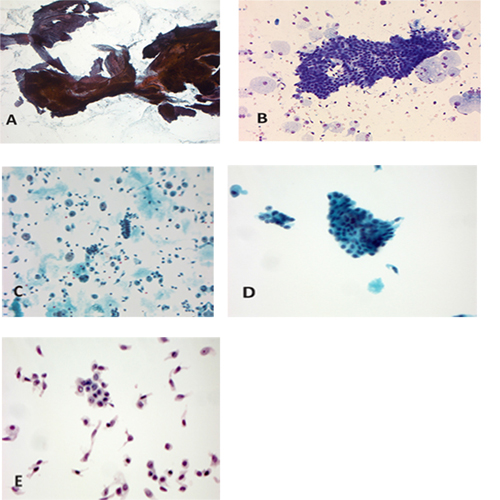
Figure 1: Benign papilloma.
a. Magnification x 50, PAP. Large and partly folded sheets of benign ductal cells in benign papilloma. b. Magnification x 200, MGG. Monolayer sheet benign ductal cells. In the background some cystic debris and macrophages
c. Magnification x 200, PAP, SurePath. Smaller groups and a short strip, debris, macrophages. d. Magnification x 400, PAP, SurePath. Micropapillary group with benign nuclear characteristics. e. Magnification x 400,PAP, ThinPrep. A distinct single cell population, but benign nuclear features, especially the fine, uniform chromatin structure. The “plain” papillomas have a moderate cellularity, sheets and groups of benign ductal cells, as well as macrophages and often also apocrine cells. These lesions are cytologically completely benign. Traditionally they are surgically excised, but some argue that it is not mandatory [22, 26]. Papeix et al found that 34/36 cases diagnosed as benign with papillary features were indeed benign papillomas and the two remaining cases were stable on radiological follow up. Proliferative lesions tend to be cellular and with a polymorph population consisting of several cell types (benign/usual intraductal hyperplasia = UDH), all with basically benign nuclear criteria (Figure 2 a-f).
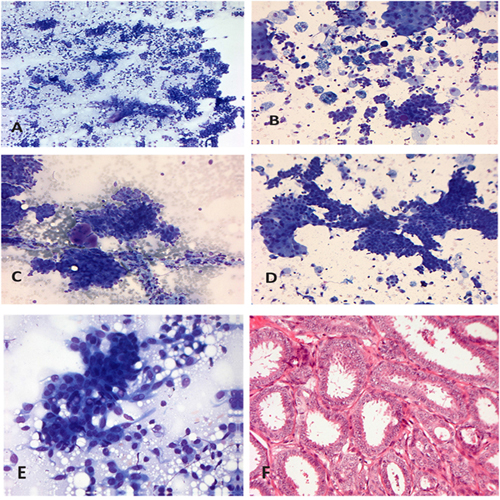
Figure 2: Cellular, benign papilloma.
a. Magnification x 100, MGG. Cellular material with stromal fragment, irregular sheets, groups and aggregates of ductal cells as well as a single cell population. b. Magnification x 200, MGG. Smaller groups and sheets, mixed ductal and apocrine as well as numerous macrophages. In addition a minor single cell population. c. Magnification x 200, MGG. Cellular papilloma with threedimensional epithelial clusters and metachromatic basement mebrane-like globules d. Magnification x 200, MGG. Complex epithelial sheets with transition from ductal to apocrine cell type. e. Magnification x 400, MGG. Cellular polymorphism in a papilloma with extensive, but histologically benign hyperplasia. Nuclear irregularities, but uniform chromatin structure. f. Magnification x 200, HE. Proliferative papilloma with adenosis; same lesion as 2e. They may harbor areas of ductal carcinoma in situ (DCIS), atypical ductal hyperplasia (ADH) or lobular neoplasia. DCIS can be both high grade and non-high grade. Cells from high grade DCIS are clearly recognized as malignant [27], whereas aggregates and single cells from a non-high grade lesions may not be definitely identified in the smears. In many cases though, the atypical cells may not present in the specimens. Immunocytochemistry can be helpful, providing there is adequate material for ICC (Table 3). These cellular and heterogeneous papillary lesions should be diagnosed as equivocal/ atypical and surgically excised.
Table 3: Overview of papillary lesions and their immunophenotypes.
| Tumor type | Benign/ malignant | p63 | High mocelular weight (HMW) cytokeratins CK5/6, CK14 | ER/PgR |
| Intraductal papilloma 1.NOS 2. with benign hyperplasia (UDH= usual ductal hyperplasia)) | benign | positive | positive in myoepithelial cells | patchy positive |
| 3. with atypical ductal hyperplasia (ADH) 4. with lobular neoplasia (ALH(atypical lobular hyperplasia)+ LCIS (lobular carcinoma in situ)) | borderline | mixed | mixed | Mixed patchy and uniform |
| 5. with ductal carcinoma in situ (DCIS) | in situ | negative | negative | uniform and 100% positive |
| Subareolar papillomatose | benign | negative | negative | uniform and 100% positive |
| 5. with ductal carcinoma in situ (DCIS) | in situ | positive | positive in myoepithelial cells | patchy positivity |
| Intraductal papillary carcinoma | in situ; usually low-grade with occasionally high grade lesions | negative in papillary areas; positive in duct periphery | negative | uniform and 100% positive |
| Intraductal papillary carcinoma | in situ; usually low-grade with occasionally high grade lesions | negative in papillary areas; positive in duct periphery | negative | uniform and 100% positive |
| “encapsulated”/ intracystic papillary carcinoma | In situ or invasive, low grade | negative | negative | uniform and 100% positive |
| Solid papillary carcinoma | In situ or invasive, low grade | negative | negative | uniform and 100% positive |
| invasive papillary carcinoma | invasive | |||
| invasive papillary carcinoma | invasive, high grade | negative | negative | usually positive |
Florid papillomatosis of the nipple (subareolar papillomatosis) is a benign epithelial proliferation localized within and around the collecting ducts of the nipple. It comprises < 1 % of breast specimens and has an age range of 20-87 yrs (mean 43 yrs). Approximately 2/3 of the women presents with nipple discharge. Some cases may have skin erosion and mimic Paget’s disease of the nipple clinically [25]. The cytologic findings are listed in (Table 4) and they are illustrated in (Figure 3 a-g). If palpable, the clinical findings are usually very characteristic and help making a confident diagnosis. The FNAC material is moderate to abundant and can be prepared both as smears, as LBC and as cell block (Figure 4 a-e). ICC phenotype (Table 2) reveal a benign, polymorph cell composition and supports the diagnosis of a benign lesion.
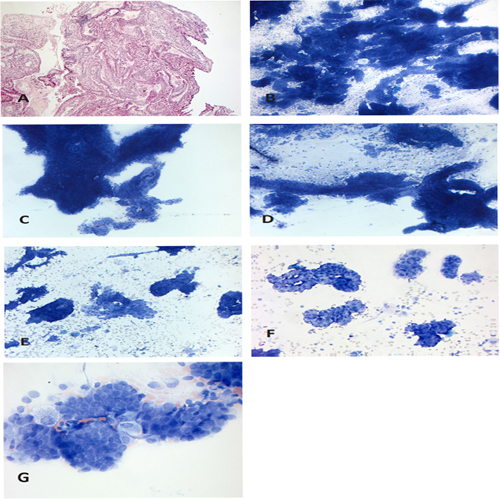
Figure 3: Subareolar papillomatosis.
a. Magnification x 50; HE, cell block. FNAC material from a cellular papillary lesion located in the nipple. b. Magnification x 50, MGG. Abundant cellularity with large, complex and folding epithelial aggregates c. Magnification x 100, MGG. Complex cohesive aggregates. d. Magnification x 100, MGG. Complex aggregate with part of the stromal papillary stalk and a minor component of single cells e. Magnification x 100, MGG. Irregular,medium sized aggregates, both ductal and apocrine. f. Magnification x 200, MGG. Micropapillary structures g. Magnification x 400, MGG. Very regular, benign nuclei with uniform chromatin structure.
Table 4: Cytologic findings in subareolar papillomatosis.
- Moderate or high cellularity with a basic benign pattern
- Small amount of debris, inflammatory cells and siderophages may be found
- Aggregates and smaller epithelial groups
- Basically cohesive, irregular aggregates
- Irregular shapes
- Micropapillary, macrophages, naked nuclei
- Uniform nuclei with finely distributed chromatin and small nucleoli
- Little anisonucleosis, occasional hyperchromatic nuclei possible
- Occasional) dispersed epithelial cells
- Apocrine cells may be present
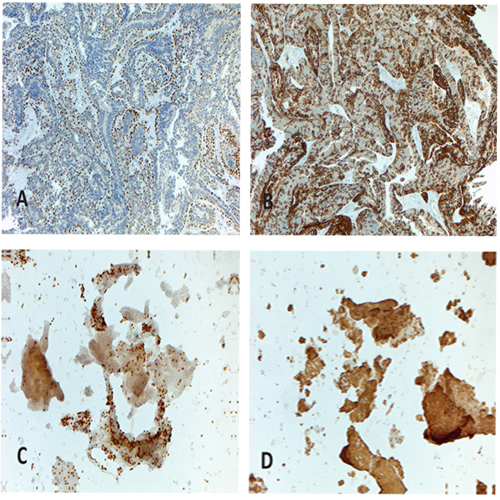
Figure 4a: subareolar papillomatosis immunophenotype. Magnification x 100, cell block stained with p63 Figure 4b: subareolar papillomatosis immunophenotype. Magnification x 100, cell block stained with CK 5/6. Figure 4c: subareolar papillomatosis immunophenotype. Magnification x 100, LBC (ThinPrep) with cytospin preparation stained with p63. Figure 4d: subareolar papillomatosis immunophenotype. Magnification x 100, LBC (ThinPrep) with cytospin preparation stained with CK 5/6.
Papillary carcinoma variants Intraductal papillary carcinoma in situ may present with a clear or blood stained nipple discharge. More peripheral lesions may present as a mass. Radiologically it can present both as a single, round and partly cystic lesion as well as micro-calcifications (as part of a DCIS) without a tumor [25]. In histology, we find ducts or TDLU (terminal duct-lobular unit) with slender branching fibro-vascular stalks covered by a single cell population of neoplastic cells (Figure 5 a-k). Micropapillary, cribriform and solid growth patterns are also seen. The papillae are lined by neoplastic, columnar cells in one or several layers. The cells are deceptively bland with low - grade atypia. The cytological findings mirror the histology and are detailed in Table 5.
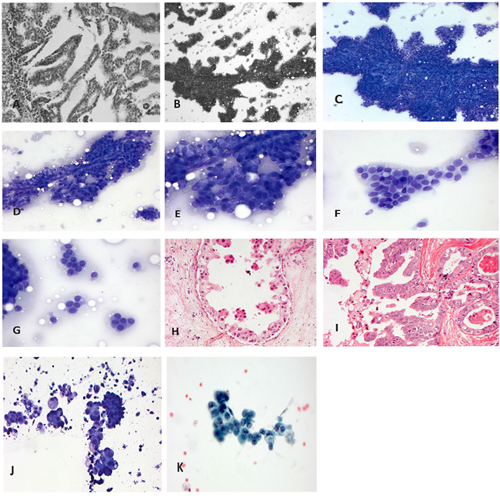
Figure 5: intraductal papillary carcinoma (papillary DCIS).
a. Magnification x 100. HE. Slender papillary structures lined by one layer of epithelial cells with low - grade nuclear atypia and delicate fibrovascular stalks b. Magnification x 50, MGG. Overview of smear with large papillary aggregate and numerous cell groups of varying sizes. c. Magnification x 100, MGG. On larger magnification the branching capillaries are seen d. Magnification x 200, MGG. A smaller papillary fragment with central capillary surrounded by low-grade atypical cells. There is mild to moderate nuclear pleomorphism and scattered single cells e. Magnification x 400, MGG. On larger magnification a fine to somewhat coarse chromatin is seen and inconspicuous nucleoli f. Magnification x 400, MGG. Micropapillary epithelial cell group with low-grade nuclear atypia g. Magnification x 400, MGG. Smaller epithelial cell groups with lowgrade nuclear atypia h. Magnification x 200, HE. Micropapillary epithelial proliferations with varying nuclear atypia, up to high grade (G1-3) i. Magnification x 200, HE. Papillary epithelial proliferation with high grade atypical nuclei (G3) j. Magnification x 400, MGG. Micropapillary DCIS G1-3 with proteineous debris, macrophages and micropapillary epithelial cell groups. One of the micropapillary groups shows a low-grade nuclear atypia whereas the rest are high grade with prominent pleomorphism k. Magnification x 400, PAP. Loosely cohesive sheet with high grade malignant cells: coarse irregularities in the nuclear contour, irregular peripheral chromatin brim, coarse nuclear chromatin with clearing and prominent nucleoli. Cytoplasmic vacuolization is seen in some of the cells.
Encapsulated papillary carcinoma [25] is a variant of papillary carcinoma characterized by fine fibrovascular cores covered by neoplastic cells of low or intermediate grade and surrounded by a thick fibrous capsule (figure 6a). In the majority of cases there are no myoepithelial cell layer within the papillae or at the periphery of the lesion. There is a circumscribed round mass on mammography and ultrasound imaging. A frank invasive component is usually IDC and cannot be appreciated in the cytological material. Nipple discharge may be present. Cytologically the features (Figure 6b-g) are the same as the intraductal papillary carcinoma (Table 5), and the two entities can only be distinguished histologically.
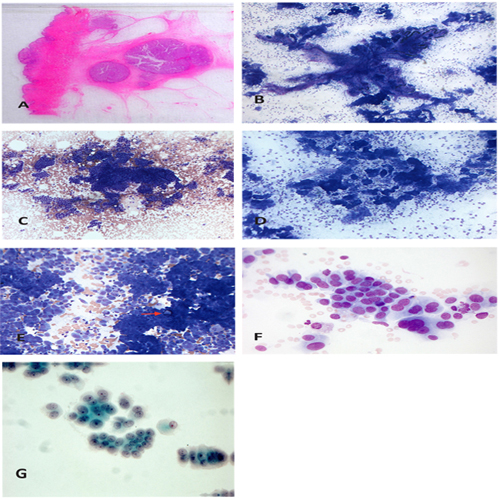
Figure 6: Encapsulated, papillary carcinoma.
a. Magnification x 10, HE. Well demarcated papillary carcinoma (the two central nodules). In addition an ordinary invasive ductal carcinoma to the right and above. b. Magnification x 50, MGG. Overview with large, branching papillary aggregate as well as smaller groups c. Magnification x 100, MGG. Monolayer (two-dimensional) sheets as well as a complex partly three-dimensional and partly monolayer aggregate. In additon we can see numerous single cells and some “strips” d. Magnification x 100, MGG. Numerous micropapillary cell groups e. Magnification x 200, MGG. The cells groups are loosely cohesive with numerous single cells. There is a mild to moderate pleomorphism. Microcalcification (arrow). f. Magnification x 400, MGG. A loosely cohesive sheet with nuclei in the size range of 2-3 X RBC. g. Magnification x 630, PAP, ThinPrep. Small epithelial groups with low - grade nuclear atypia. The nuclear chromatin is finely granular with accentuated peripheral chromatin brim and there are small to medium sized nucleoli.
Table 5: Cytological features of papillary carcinomas (intraductal, encapsulated and solid).
- May be cystic on aspiration
- Cell material is usually abundant
- Epithelial cells are monotonous and appear “monoclonal” showing low grade nuclear/cell atypia (usually G1)
- Anisonucleosis, hyperchromasia, coarse chromatin and prominent nucleoli are uncommon (occasionally G2-G3).
- Benign bipolar cells are absent from the background, myoepithelial cells are not seen within the groups or are very scarce
- Large papillary cell clusters forming arborizing arrays bearing overlapping, palisaded cells on a fibrovascular core may be present (as in papilloma)
- Cells may be dispersed and the fibrovascular cores denudeds
- (pseudo)-papillary arrangement of cells (in the solid-papillary type )
- micropapillary as well as irregular small epithelial cell groups
- The epithelial cells are often distinctly columnar in appearance
- Evaluation of invasive component not possible
- Microcalcifications are common findings
- Intracytoplasmic vacuoles are not rare
- neuroendocrine differentiation common in solid-papillary type
- Often extensive dissociation in single cells, plasmacytoid
Solid papillary carcinoma [25] represents < 1 % of breast carcinomas. It occurs usually in menopausal women with a mean in the seventh decade. About 20-25 % have a bloody discharge. Mammography may show an abnormality or lobular lesion. Ultrasound may also show a lobulated mass that histologically (Figure 7a,b) corresponds to closely apposed, expansile nodules with delicate fibrovascular cores within the nodules. These tumors often reveal neuroendocrine differentiation and/or mucinous components. Conventional invasive growth may be present, often having mucinous or neuroendocrine features [28, 29]. The cytological features resemble the two above subtypes of papillary carcinomas (Table 5) (Figure 7c-h). The cystic component is virtually absent, and debris and macrophages are not present. The features and findings of the epithelial cells, though, are virtually the same as the two above. Images illustrating the findings are seen in figures 7c-h. The cytological criteria are those of a low - grade carcinoma [28]. The presence of an eventual additionally invasive component cannot be evaluated in these three lesions. Primary surgery should then be complete excision, but should not include removal of the sentinel node (SN) or extensive surgery An overview and comparison of cytological features and immunocytochemical findings in benign and malignant papillary lesions is given in tables 3 and 6.
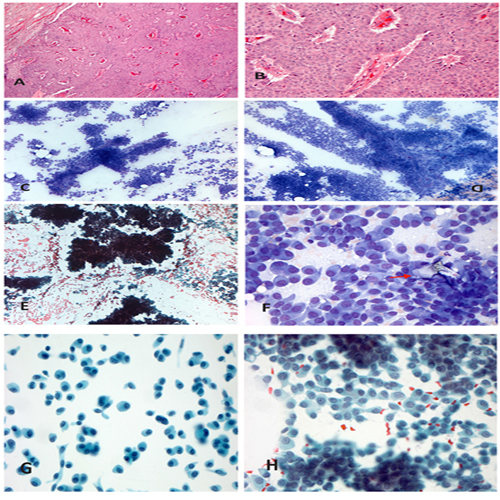
Figure 7: Solid-papillary carcinoma.
a. Magnification x 50, HE. Solid growing carcinoma with a well demarcated border b. Magnification x 200, HE. Low -grade nuclear atypia and intratumoral branching vessels. c. Magnification x 100, MGG. Abundant cell material with large, pseudopapillary and three-dimensional epithelial aggregates, smaller groups and a large single cell population d. Magnification x 100, MGG. Loosely cohesive cells with abundant single cells e. Magnification x 100, PAP. Large, three-dimensional aggregates, loosely cohesive cells f. Magnification x 400, MGG. Loosely to non- cohesive, low-grade carcinoma cells with plasmacytoid appearance. Microcalcification (arrow). g. Magnification x 400, PAP, SurePath. Mainly single cell population of plasmacytoid cells with delicate, finely granular chromatin and small, but visible nucleoli h. Magnificatin x 400, PAP. Abundant, loosely cohesive and plasmacytoid cells. The chromatin if fine granular, but more distinct than in the SurePath preparation. Nucleoli are small, but distinct
Table 6: Morphologic - diagnostic considerations cellular (benign) papillary lesions versus papillary carcinoma.
| (Benign) cellulary papillary lesion | Papillary carcinoma (in situ and/or invasive) ( |
| heterogeneous (“polyclonal”) cell population | monomorphous (“monoclonal”) cell population |
| basic benign pattern, but may have a population of cells showing low grade nuclear atypia/anisonucleosis | low grade nuclear atypia in the vast majority of cases |
| straight or curved tubular structures representing adenosis in papilloma | |
| mostly cohesive, but with single cells | more discohesive, often extensive |
| threedimensional cells aggregates representing/resembling low grade DCIS, solid and/or cribriform | threedimensional cells aggregates representing/resembling low grade DCIS, solid and/or cribriform |
| papillary and micropapillary groups | papillary and micropapillary groups |
| fibrovascular stalks | fibrovascular stalks |
| fdebris and macrophages | debris and macrophages |
Invasive micropapillary carcinomas [25] are composed of small, hollow and morula-like clusters of cancer cells and sur- rounded by clear stromal places (Figure 8a). There is usually a reversed polarity, an “in side out” growth pattern, whereby the apical pole of the cells faces the stroma and not the luminal surface. They make up 0.9-2 % of invasive breast cancers [4], but up to 7.4 % off invasive breast cancers may have partial micropapillary growth pattern [5]. The mean age is as in IDC, 75 % are grade 2 and 3, estrogen and progesterone receptors (ER/PgR) are usually positive, whereas HER-2 is variable, but often positive. They usually present as a palpable mass. Cytologically these present as high grade carcinoma cells in well demarcated, angulated micropapillary groups lacking a fibrovascular core with irregular crowded nuclei (Figure 8b-d) and are clearly malignant [30-32]. According to the WHO (world health organization) definition [25], invasive papillary carcinoma is a tumor with predominantly papillary growth pattern (> 90 %) in the invasive component. It is a rare tumor with no known clinical characteristics or known epidemiological data. The tumor resembles papillary carcinomas from other organ sites, in particular ovary, tube and lung that are the main differential diagnoses. The cytological features have not been described.
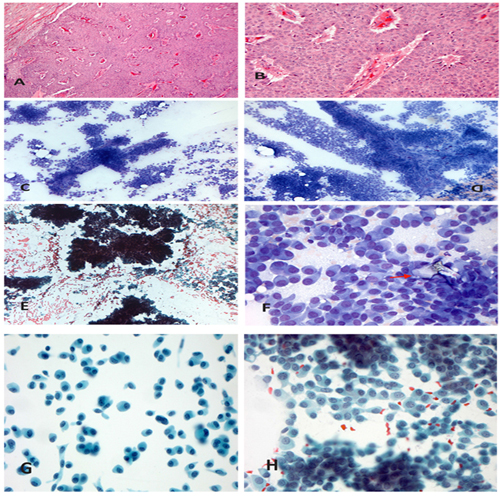
Figure 8: Invasive, micropapillary carcinoma.
a. Magnification x 400, HE. Micropapillary carcinoma groups with high grade nuclear atypia (G3) b. Magnification x 100, MGG. Numerous micropapillary epithelial cell groups c. Magnification x 100, PAP. Numerous micropapillary epithelial cell groups d. Magnification x 400, PAP. High grade nuclear atypia with coeaarse chromatin, distinct nuclear size variation and in conspicious nucleoli e. Magnification x 400, MGG. High grade atypical cells in micropapillary arrangement; clearly irregular nuclear contour and irregular chromatin. Nuclear size is 4-5x RBC.
REFERENCES
- Aggarwal D, Soin N, Kalita D, Pant L, et al. (2014). Cytodiagnosis of papillary carcinoma of the breast: Report of a case with histological correlation. J Cytol. 31(2): 119-121.
- Choi YD, Gong GY, Kim MJ, Lee JS, et al. (2006). Clinical and cytologic features of papillary neoplasms of the breast. Acta Cytol. 50(1): 35-40.
- Gomez-Aracil V, Mayayo E, Azua J, and Arraiza A. (2002). Papillary neoplasms of the breast: clues in fine needle aspiration cytology. Cyopathology. 13(1): 22-30
- Hardisson D, González-Peramato P, Perna C, Cuevas J, et al. (2003). Fine needle aspiration cytology of solid papillary carcinoma of the breast. A report of four cases. Acta Cytol. 47(2): 259-264.
- Nayar R, De Frias DV, Bourtsos EP, Sutton V, et al. (2001). Cytologic differential diagnosis of papillary pattern in breast aspirates: correlation with histology. Ann Diagn Pathol. 5(1): 34-42.
- Weigner J, Zardawi I, Brave S and McElduff P. (2015). The conundrum of papillary breast lesions within the C3 category. Acta Cytol. 59(4): 289-297.
- Bardales RH, Suhrland MJ and Stanley MW. (1994).Papillary neoplasms of the breast: fine-needle aspiration findings in cystic and solid cases. Diagn Cytopathol. 10(4): 336-341.
- Corkill ME, Sneige N, Fanning T and el-Naggar A. (1990). Fine needle aspiration cytology and flow cytometry of intracystic papillary carcinoma of breast. Am J Clin Pathol. 94(6): 673-680
- Dei Tos AP, Della Giustina D and Bittesini L. (1992). Aspiration biopsy of malignant papillary breast neoplasms. Diagn Cytopathol. 8(6): 580-584.
- Jayaram G, Elsayed EM and Yaccob RB. (2007). Papillary Breast Lesions Diagnosed on Cytology. Acta Cytol. 51(1): 3-8.
- Kumar PV Talei AR, MS, MA, et al. (1999). Papillary carcinoma of the breast. Cytologic study of nine cases. Acta Cytol. 43(5): 767-770
- Jeffrey PB and Ljung BM. (1994). Benign and malignant papillary lesions of the breast. Am J Clin Pathol. 101(4): 500-507
- Mockli G, Hanks D and Jeffrey PB. (1993).Papillary carcinoma of the male breast: report of a case diagnosed by fine needle aspiration. Acta Cytol. 37(5): 721-724
- Naran S, Simpson J and Gupta RK. (1988). Cytologic diagnosis of papillary carcinoma of the breast in needle aspirates. Diagn Cytopathol. 4(1): 33-37
- Prathiba D, Shalinee Rao, Kasthuri Kshitija, and Leena Dennis Joseph. (2010).Papillary lesions of breast – An introspect of cytomorphological features. J Cytol. 27(1): 12-15.
- Reid-Nicholson MD, Tong G, Cangiarella JF and Moreira AL. (2006). Cytomorphologic features of papillary lesions of the male breast: a study of 11 cases. Cancer. 108(4): 22-30
- Nguyen GK and Redburn J. (1992). Aspiration biopsy cytology of papillary carcinoma of the breast. Diagn Cytopathol. 8(5): 511-516.
- Simsir A, Waisman J, Thorner K and Cangiarella J. (2003). Mammary Lesions Diagnosed as “Papillary” by Aspiration Biopsy. Cancer Cytopathol. 99(3): 156-165.
- Tse GM, Ma TK, Lui PC, Ng DC, et al. (2008). Fine needle aspiration cytology of papillary lesions of the breast: how accurate is the diagnosis? J Clin Pathol. 61(8): 945-949.
- Haji BE, Das DK, Al-Ayadhy B, Pathan SK, et al. (2007). Fine-needle aspiration cytologic features of four special types of breast cancers: mucinous, medullary, apocrine, and papillary. Diagn Cytopathol. 35(7): 408-16
- Michael CW and Buschmann B. (2002). Can True Papillary Neoplasms of Breast and Their Mimickers Be Accurately Classified by Cytology? Cancer Cytopathol. 96(2): 92-100.
- Field A and Mak A. (2007). A prospective study of the diagnostic accuracy of cytological criteria in the FNAB diagnosis of breast papillomas. Diagn Cytopathol. 35(8): 465-475
- Jayaram G, EE and Yaccob RB. (2007). Papillary Breast Lesions Diagnosed on Cytology. Acta Cytol. 51: 3-8.
- Myers T and Wang HH. (2000). Fibroadenoma mimicking papillary carcinoma on ThinPrep of fine-needle aspiration of the breast. Arch Pathol Lab Med. 124(11): 1667-1669.
- Lakhani SR EI, Schitt SJ, Tan PH, van de Vivjer M. (2012). WHO classification of tumours of the breast. 4 ed. Bosman FT JE, Lakhani SR, Ohgaki H, editor. Lyon, France: International Agency for Research of Cancer.
- Papeix G, Zardawi IM, Douglas CD, Clark DA, et al. (2012). The Accuracy of the ‘Triple Test’ in the Diagnosis of Papillary Lesions of the Breast. Acta Cytol. 56(1): 41-46.
- Sauer T, Lømo J, Garred Ø and Næss O. (2005). Cytologic features of ductal carcinoma in situ in fine-needle aspiration of the breast mirror the histopathologic growth pattern heterogeneity and grading. Cancer Cytopathol. 105(1): 21-27.
- Hardisson D, González-Peramato P, Perna C, Cuevas J, et al. (2003). Fine needle aspiration cytology of solid papillary carcinoma of the breast. A report of four cases. Acta Cytol. 47(2): 259-264
- Tse, GM and MT. (2000). Fine-needle aspiration cytology of breast carcinoma with endocrine differentiation. Cancer. 90(5): 286-291
- Bayramoglu H, ZO, Erhan Y, Ciris M, et al. (2002). Fineneedle aspiration biopsy of invasive micropapillary carcinoma of the breast: a report of five cases. Diagn Cytopathol. 27(4): 214-217
- Khurana KK, Wilbur D and Dawson AE. (1997). Fine needle aspiration cytology of invasive micropapillary carcinoma of the breast. Acta Cytol. 41: 1394-1398.
- Wong S, CH and Tse GM. (2000). Fine needle aspiration cytology of invasive micropapillary carcinoma of the breast. Acta Cytol. 44: 1085-1089.