Previous Issues Volume 1, Issue 2 - 2016
Subarachnoid Hemorrhage in Association with Heroin Overdose
Alan Lucerna1, 2, James Espinosa1
1Department of Emergency Medicine, Rowan University SOM Kennedy University Hospital, Stratford, NJ, USA.
2Program director of the combined Emergency Medicine/Internal Medicine at Rowan University SOM Kennedy University Hospital in Stratford, NJ, USA.
Corresponding Author: James Espinosa, Department of Emergency Medicine, Rowan University SOM Kennedy University Hospital, 18 East Laurel Road, Stratford, NJ 08084, USA, Tel: +1 646 241 5695; E-Mail: [email protected]
Received Date: 10 Mar 2016 Accepted Date: 27 Jun 2016 Published Date: 30 Jun 2016
Copyright © 2016 Espinosa J
Citation: Lucerna A and Espinosa J. (2016). Subarachnoid Hemorrhage in Association with Heroin Overdose. Mathews J Emergency Med. 1(2): 011.
ABSTRACT
We present a case of bilateral diffuse subarachnoid hemorrhage without intraventricular extension, identified on the head CT in association with heroin use. Such an association has been rarely reported in the literature.
KEYWORDS
Subarachnoid Hemorrhage in Association with Heroin Overdose; Subarachnoid Hemorrhage and Association with Heroin Overdose; Neurological Consequences of Drug Abuse; Neurological Consequences and Drug Abuse; Stroke and Drug Abuse; Stroke and Heroin Abuse.
INTRODUCTION
The intravenous use of heroin may cause cardiopulmonary arrest, with the consequence of post-hypoxic encephalopathy and other systemic consequences of hypoxia. Strokes in association with heroin may occur by a number of mechanisms. However, heroin does not elevate blood pressure. Hemorrhages in association with heroin use may be caused by infective arteritis/mycotic aneurysm. We present a case of bilateral diffuse subarachnoid hemorrhage without intraventricular extension, identified on the head CT, in association with heroin use. Such an association has been rarely reported in the literature. It may be underreported due to attribution of the death to heroin overdose.
CASE PRESENTATION
A 39 year old male presented to the hospital status-post cardiac arrest. The patient was found by his mother. He had a syringe in his hand. The patient was reportedly a heroin user but has no other pertinent medical issues. The patient, who lived with his mother, was last seen the night before. The patient's mother, a registered nurse, noted the patient to be unresponsive, with gray skin coloring and with no pulses. His mother administered intranasal naloxone, called 911 and administered cardiopulmonary resuscitation (CPR). The emergency management system (EMS) team reported that the patient was in asystole. The patient was subsequently intubated and was after given one dose of epinephrine. He then had return of spontaneous circulation but remained unconscious with a Glasgow Coma Scale of 3. His initial clinical course was complicated by hypotension with systolic blood pressures in the 50 to 60 mm Hg range. His blood pressure eventually stabilized with the administration of intravenous fluids and vasopressors. The ECG showed normal sinus rhythm with a rate of 81 with a normal axis. An intraventricular conduction delay was noted with a QTc (Bezet) of 497 ms. First troponin was 0.03. The complete blood count revealed a white blood cell count of 14.3x10*3/uL with normal hemoglobin and platelets. The basic metabolic panel showed the following: sodium of 141 mmol/L, potassium of 5.6 mmol/L, chloride of 103 mmol/L, CO2 16 mmol/L, BUN of 11 mg/dL and creatinine of 1.73 mg/ dL. The ALT was 245 U/L and the AST was 291 U/L. The lipase was 50. The lactic acid was very elevated at 14.3 mmol/L. The patient's urine drug screen was positive for opiates only. The alcohol level was negative. Severe acidosis was noted in the ABG with arterial PH of 6.90, [PCO2 of 71, PO2 of 213, HCO3 of 12, BE of -22.6, and measured saturation of 100% on 100% FIO2. The chest X-ray did not show any infiltrates or pneumothorax and the cardiomediastinal silhouette was normal in size. The endotracheal tube and nasogastric tube were in good position. Prior to the induction of hypothermia, the patient was sent for a CT scan of the head, cervical spine, chest, abdomen and pelvis. Bilateral diffuse subarachnoid hemorrhage without intraventricular extension was identified on the head CT (Figure 1).
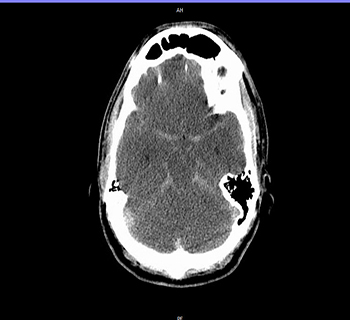
Figure 1: CT scan, head, showing findings consistent with cerebral edema and subarachnoid haemorrhage.
No fractures were noted on head CT. Additionally, there was a complete loss of the gray-white matter differentiation with diffuse sulcal effacement consistent with anoxic brain injury and cerebral edema. No midline shift was noted, but there was a mass effect on the left lateral ventricle (Figure 2).
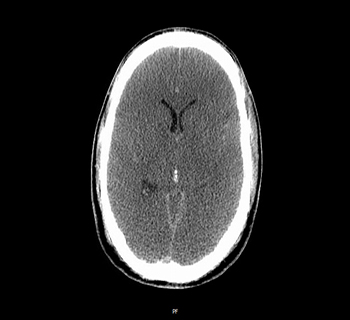
Figure 2: CT scan, head, shows no midline shift. Mass effect noted left lateral ventricle.
The cervical spine showed no fractures or dislocation. The CT of the abdomen showed diffuse small and large bowel wall thickening with adjacent inflammatory changes likely related to hypotensive episode (Figure 3).
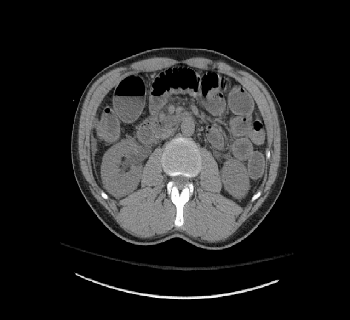
Figure 3: CT scan, abdomen, showing diffuse small and large bowel thickening.
There was also periportal, pancreatic, and renal edema. Given the results the patient was felt not to be a candidate for hypothermia. A neurosurgical consultation was obtained and the patient was transferred to a neurosurgical unit. The patients Hunt-Hess score was 5. The patient was subsequently sent for a Nuclear Study to evaluate brain vascular flow. There was no activity seen within the brain or intracranial vascular structures. The "hot nose" sign was clearly present indicative of shunting from the internal carotid to external carotid artery vascular structures (Figure 4). These findings were consistent with brain death.

Figure 4: Nuclear study, brain, showing the "hot nose" sign. A lack of activity is noted within the brain and intracranial vascular structures.
DISCUSSION
In this case, heroin use was associated with bilateral diffuse subarachnoid hemorrhages in the absence of physical or radiographic signs of trauma. There was evidence of opiates on the UDS. There was a history of heroin use. The abdominal CT findings of diffuse small and large bowel wall thickening with adjacent inflammatory changes in the presence of periportal, pancreatic, and renal edema would seem consistent with hypotension. Similarly, the head CT findings of complete loss of the gray-white matter differentiation with diffuse sulcal effacement consistent is consistent with anoxic brain injury and associated cerebral edema. However, the finding of bilateral diffuse subarachnoid hemorrhage without intraventricular extension, identified on the head CT, has not been extensively reported in association with heroin use. In fact, it appears that such an association has been rarely reported. Sloan et al looked at data from the Maryland Stroke Data Bank. In reference to the question of ischemic or hemorrhagic stroke in temporal association with drug abuse, stroke associated with drug use occurred in 7% of subarachnoid hemorrhages. Drugs implicated in hemorrhagic or ischemic stroke included heroin [1]. DiLuna et al reported the case of a 54 year old female with a diffuse subarachnoid hemorrhage. The patient was noted by her family to have been injecting "into her neck" because of poor peripheral access. The authors found an internal carotid dissection with a fusiform aneurysm with vertebral dissection with a vertebral puncture site injury. The underlying pathogenesis was felt to be "either abscess or endarteritis and local thrombosis or vasospasm and inflammation from mural injury" [2]. Amine et al presented a case of brain abscess and a case of brain mycotic aneurysm in association with heroin use. They concluded that few neurosurgical complications occur from heroin use [3]. Guner et al presented a very interesting case of a subarachnoid hemorrhage in association with heroin use. In their case, heroin-induced subarachnoid hemorrhage was identified in a patient who had angiographic evidence of typical moyamoya vasculopathy. It was felt the heroin induced the moyamoya vasculitis [4]. In a review of recreational drugs and their neurological consequences, Enevoldson makes a number of points that appear to attend to this case. In his discussion of heroin, he points out that the intravenous use of heroin may cause cardiopulmonary arrest, as was seen in this case. "Post-hypoxic encephalopathy is therefore one of the more frequent effects of heroin abuse seen by the neurologist." In reference to strokes, Enevoldson notes that strokes may occur by a number of mechanisms. However, heroin does not elevate blood pressure [5]. "Hemorrhages should be assumed to be caused by infective arteritis/mycotic aneurysm until proven otherwise." Thus it may be that the cases presented by DiLuna, Amine and Guner might all be related to underlying heroin-associated vasculitis. It appears that post-hypoxic injury was seen in this case. However, the presence of bilateral subarachnoid hemorrhages has been rarely reported in the literature. The relationship of these hemorrhages to a vasculitis, as discussed by Enevoldson, is an intriguing question that was neither proved nor disproved in the case presented.
CONCLUSION
We present a case of bilateral diffuse subarachnoid hemorrhage without intraventricular extension, identified on the head CT in association with heroin use. Such an association has been rarely reported in the literature. It may be underreported due to attribution of the death to heroin overdose. The intravenous use of heroin may cause cardiopulmonary arrest, with the consequence of post-hypoxic encephalopathy and other systemic consequences of hypoxia. Strokes in association with heroin may occur by a number of mechanisms. However, heroin does not elevate blood pressure. Hemorrhages in association with heroin use may be caused by infective arteritis/mycotic aneurysm.
REFERENCES
- Sloan MA, Kittner SJ, Rigamonti D and Price TR. (1991). Occurrence of stroke associated with use/abuse of drugs. Neurology. 41(9), 1358-1364.
- DiLuna ML, Bydon M, Gunel M and Johnson MH. (2007). Neurological picture. Complications from cervical intra-arterial heroin injection. J Neurol Neurosurg Psychiatry. 78(11), 1198.
- Amine AR. (1977). Neurosurgical complications of heroin addiction: brain abscess and mycotic aneurysm. Surg Neurol. 7(6), 385-386.
- Guner S, Ersin O, Onur S, Hakan M, et al. (2008). Case Report: Heroin Induced Subarachnoid Hemorrhage in Moyamoya Disease: Anatol J Clin Investig. 2(1), 31-33.
- Enevoldson T. (2004). Recreational drugs and their neurological consequences. J Neurol Neurosurg Psychiatry. 75(Suppl 3), iii9-iii15.