Information Links
Related Conferences
Previous Issues Volume 5, Issue 1 - 2022
Serum Laboratory Biomarkers to Estimate the Probability of Complicated Appendicitis: CRP and LDH
Dr. Peyman Virani1, Dr. Ozra Nouri2, Dr. Ali Farbod1, Mahshid Dehghan2, Aisan Akhgari2*, Zahra Javadpour Ebrahim2
1Surgery Department, Tabriz University of Medical Sciences, Tabriz, Iran
2Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
Received Date: April 16, 2022
Published Date: May 12, 2022
*Corresponding author: Aisan Akhgari, Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran. Tel: +989142958117; E-mail: [email protected]
Citation: Akhgari Aisan, et al. (2022). Serum laboratory biomarkers to estimate the probability of complicated appendicitis: CRP and LDH. Mathews J Surg. 5(1):15.
Copyright: Akhgari Aisan, et al. © (2022).
ABSTRACT
Objective: Acute inflammation of the appendix is a very common finding in patients representing the emergency department. Here, we assessed the levels of the serum laboratory biomarkers in the patients with complicated (defined by the presence of perforation, abscess, or peritonitis) and simple appendicitis. Methodology: This observational study was conducted in Sina Hospital, Tabriz-Iran, between March 2019 and August 2019. Data regarding age, sex, body temperature, length of hospital stays, clinical signs and symptoms, and time of symptom onset for each patient. Laboratory values including white blood cells (WBC) count, neutrophil percentage, erythrocyte sedimentation rate (ESR), C-reactive protein (CRO), mean platelet volume (MPV), and lactate dehydrogenase (LDH) were evaluated. Results: A total of 279 patients were enrolled in the study. 131 patients (46.9%) had complicated and 148 (53.0%) had simple appendicitis. Mean body temperature (P-value 0.05). There were no significant differences regarding WBC, neutrophil, 1st and 2nd hour ESR, MPV, and LDH levels, and mean length of hospital stay (P-value>0.05). Conclusion: CRP concentrations are reliable markers showing an increased risk of developing complications in acute appendicitis patients.
Keywords: Acute appendicitis; complicated appendicitis; lactate dehydrogenase, C-reactive protein; laboratory biomarkers
INTRODUCTION
Acute inflammation of the appendix, known as appendicitis, is a very common finding in patients representing the emergency department with abdominal pain. Men and women have a lifetime risk of 8.6% and 6.7%, for appendicitis, respectively. The incidence of this condition is the highest in the second decade of life [1,2]. Patients with acute appendicitis show a variety of symptoms, creating a wide range of differential diagnoses. Furthermore, there's an overlap between symptoms of appendicitis and conditions such as gastritis, abdominal lymphadenitis, ovarian cysts, acute salpingitis, intestinal and urinary infections, and nephrolithiasis, which makes the diagnosis problematic. Considering that many of the above conditions do not require surgery, distinguishing appendicitis from other differential diagnoses is important. 1/3 of patients with appendicitis show classic symptoms including abdominal pain (generalized at first but localizing in right lower quadrant after hours), nausea, and vomiting. In the case of neglecting and delaying in diagnosis, it can progress to perforation, peritonitis, and septic shock, leading to an increased death risk [3-5].
The diagnosis of this condition is based on clinical findings; right lower quadrant pain, gastrointestinal symptoms (starting after the onset of pain), leukocytosis and neutrophilia, increased C-reactive protein (CRP) concentration, and fever are considered diagnostic of appendicitis. Alvarado score (Developed by Alvarado in 1986 for the diagnosis of acute appendicitis in an emergency) can help improve diagnostic accuracy. Currently, the standard treatment of this condition is appendectomy [2,3].
Lactate Dehydrogenase (LDH) is a soluble cytoplasmic enzyme that is present in almost all cells. It's released in the extracellular space in the case of plasma membrane damage [6]. According to the literature, the pathogenesis of appendicitis consists of the generation of free radicals and the triggering of inflammatory reactions. Previous studies have shown low levels of antioxidants in patients with acute appendicitis, and an associated elevated level of oxidative stress and lipid peroxidation in the blood. Therefore, the generation of free radical and the resulting stress has an important role to play in the underlying pathogenesis [7-10]. Therefore, elevated levels of LDH, as an important marker of oxidative stress and cell death, maybe a diagnostic parameter in diagnosing acute appendicitis.
Here, to find anticipating biomarkers of complicated appendicitis cases in order for on-time intervention, we assessed the levels of the serum laboratory biomarkers in the patients with complicated (defined by the presence of perforation, abscess, or peritonitis) and simple appendicitis. We hypothesized an increased level of the inflammatory biomarkers and especially LDH, in the patients with more critical and complicated statuses.
METHODS AND PATIENTS
- Study design and participants: This observational study was conducted in Sina Hospital affiliated with Tabriz University of Medical Sciences between March 2019 and August 2019 (for 6 months). Every eligible case of acute appendicitis who was admitted in the surgery ward between the given period was enrolled in the study.
Inclusion criteria were common characteristics of acute appendicitis according to the Alvarado scoring system (anorexia, nausea, and vomiting, tenderness in right lower quadrant (RLQ), etc.) and informed consent. Exclusion criteria consisted of any other diagnosis of acute abdomen, systemic diseases which increase LDH levels of serum, corticosteroid therapy, waiting for an interval appendectomy, and patient’s unwillingness to participate in the study.
- Sampling and monitoring of participants: After approval of the study protocol by the ethics committee of the Tabriz University of Medical Science, sampling was started. The convenience sampling method was used. For this, patients who were admitted to the surgery ward of Sina Hospital in Tabriz-Iran and were diagnosed with acute appendicitis were assessed in terms of eligibility criteria. If the patients met the eligibility criteria and were interested in participating in the research, the objectives and methods of study were explained to them. Also, they were assured that their information would remain confidential with the researcher. 290 patients were included and 279 of them satisfied the exclusion and inclusion criteria. The participants were followed up until after appendectomy and laboratory values and histopathological results were recorded in a checklist.
- Data collection tool: A researcher-made checklist was used to record data. This checklist included items regarding patient demographic information such as age, sex, body temperature, length of hospital stays, clinical signs and symptoms, and time of symptom onset for each patient.
Clinical examination and history taking were done. Afterward, an abdominal ultrasound study was performed on all of the patients. After establishing appendicitis diagnosis, and before performing the surgery, blood samples of the patients were collected for laboratory investigations including WBC count, neutrophil percentage, erythrocyte sedimentation rate (ESR), CRP, mean platelet volume (MPV), and LDH. To diagnose the further complications of acute appendicitis, after confirming the diagnosis of appendicitis, patients underwent appendectomy and a biopsy of the appendix was taken and sent for histopathological examination.
Regarding surgical methods, depending on the decision of the surgeon, a laparoscopic or open appendectomy was performed. In the case of hemorrhage or leakage risk and cases with gangrenous change, perforation, or formation of abscess, drainage tubes were inserted. Based on surgical or pathologic findings, cases with gangrenous change, perforation, or abscess formation were classified as complicated, and the others were classified as simple appendicitis.
- Statistical analysis: The data were analyzed using IBM SPSS statistics version 22.0 statistical analysis software (SPSS INC., IBM Corporation, Chicago, IL). Normal data distribution was examined using the Kolmogorov-Smirnov test. Quantitative data with a normal distribution, are presented as mean ± Standard Deviation (SD) and quantitative data without a normal distribution, as mode. Chi-Square Test was used to examine the relationship between qualitative data, and independent t-test was used to examine the relationship between quantitative data with normal distribution, Mann–Whitney U test for quantitative data without normal distribution, and Fisher's exact test was used in the analysis of contingency tables. Spearman correlation coefficient was used to examine the relationship between qualitative data considering the non-normal distribution of the LDH variable. A P-value less than 0.05 was considered to establish a statistically significant relationship.
RESULTS
1. Subject Characteristics
A total of 279 patients were enrolled in the study. Based on histopathological examination, of all cases 131 (46.9%) were reported as complicated and 148 (53.0%) as simple appendicitis (control group). The mean age of all patients was 30.86 ± 0.54 years with a range of 17-50. 147 patients were male (52%), and 132 were female (48%) (Table 1).
No statistically significant difference was found regarding demographic characteristics.
The mean body temperature of all patients was 37.44 ± 0.54 degrees Celsius (range, 36.8-38.5). 38 ± 0.01 (range, 37.15-38) and 37 ± 0.11 (range, 37-37.37) were mean body temperatures of the complicated appendicitis group and control group, respectively. Significant statistical difference was observed among the two groups; the body temperature of complicated appendicitis patients was notably higher than simple appendicitis patients (P-value <0.05).
The mean length of hospital stay for the complicated appendicitis group was 3.48 ± 0.02 days (range, 2.5-4) and for the control group it was reported 3.03 ± 0.10 days (range, 2-4) which showed no significant difference, statistically (P-value >0.05). No other significant differences were noted regarding basic characteristics (P-value <0.05) (Table 1).
Table 1: Demographic data of patients, complicated appendicitis vs. control group (mean ± SD and percentage)
|
|
Complicated appendicitis (n=131) |
Uncomplicated appendicitis (Control group) (n=148) |
P-value |
|
|
Age (years) (mean ± SD) |
32.47 ± 11.72 |
29.81 ± 10.08 |
0.281 |
|
|
Sex, N (%) |
Female |
61 (46.5%) |
71 (47.9%) |
0.489 |
|
Male |
70 (53.4%) |
77 (52.0%) |
||
|
Nausea, N (%) |
Positive |
77 (58.7%) |
84 (56.7%) |
0.122 |
|
Negative |
54 (41.2%) |
64 (43.2%) |
||
|
Vomiting, N (%) |
Positive |
71 (54.1%) |
78 (52.7%) |
0.427 |
|
Negative |
60 (45.8%) |
70 (47.2%) |
||
|
RLQ pain, N (%) |
Positive |
80 (61.0%) |
97 (65.5%) |
---- |
|
Negative |
51 (38.9%) |
51 (34.4%) |
||
|
Anorexia, N (%) |
Positive |
72 (54.9%) |
77 (52.0%) |
0.210 |
|
Negative |
59 (45.0%) |
71 (47.9%) |
||
|
RLQ tenderness, N (%) |
Positive |
78 (59.5%) |
90 (60.8%) |
0.471 |
|
Negative |
53 (40.4%) |
58 (39.1%) |
||
|
Accompanying disease, N (%) |
Positive |
51 (38.9%) |
51 (34.4%) |
---- |
|
Negative |
80 (61.0%) |
97 (65.5%) |
||
|
Body temperature (mean ± SD) |
38 ± 0.01 |
37 ± 0.11 |
0.025 |
|
|
Length of hospital stay (mean ± SD) |
3.48 ± 0.02 |
3.03 ± 0.10 |
0.113 |
|
2. Biomarkers levels
CRP levels in patients with complicated appendicitis were significantly higher than in the control group (P-value <0.0001). CRP levels were in the range of 38-69.2 in the complicated appendicitis group and 22.75-55.25 in the control group. There were no significant differences among the two groups regarding WBC, neutrophil, 1st and 2nd hour ESR, and MPV levels (Table 2).
Mean LDH levels in complicated appendicitis patients were 361.61 ± 149.75 and 322.7 ± 129.72 in the control group; resulting in no significant difference (P-value= 0.073) (Table 2).
Table 2: Serologic analysis of patients, complicated appendicitis vs. control group (mean ± SD)
|
|
Complicated appendicitis (n=33) |
Uncomplicated appendicitis (Control group) (n=50) |
P-value |
|
WBC count (mean ± SD) |
13630.30 ± 4992.65 |
11798 ± 3500.52 |
0.073 |
|
Neutrophil percentage (mean ± SD) |
80 ± 2.05 |
76 ± 1.80 |
0.162 |
|
1st hour ESR (mean ± SD) |
11 ± 1.00 |
11 ± 0.90 |
0.568 |
|
2nd hour ESR (mean ± SD) |
26 ± 2.02 |
24 ± 2.02 |
0.240 |
|
CRP (mean ± SD) |
59.5 ± 1.89 |
36 ± 2.03 |
< 0.0001 |
|
MPV (mean ± SD) |
9.77 ± 1.05 |
9.91 ± 1.05 |
0.578 |
|
LDH (mean ± SD) |
361.61 ± 149.75 |
322.7 ± 129.72 |
0.073 |
Mean LDH levels among male patients were 338.86 ± 123.47 with a median of 32, minimum level of 150, and maximum level of 737. Among the female patients mean LDH levels were 337.18 ±159.58 with a median of 301, minimum level of 201, and maximum level of 950; which showed no significant difference, statistically (P-value= 0.566) (Figure 1).

Figure 1: LDH level variations of patients regarding sex
To evaluate the LDH level by the age of patients, the Spearman correlation coefficient was used. Results showed a notable relationship between these two variables and older patients had lower levels of LDH (P-value= 0.046 and r= -0.222) (Figure 2).

Figure 2: Spearman’s correlation between LDH levels and patients' age
In the evaluation of the relation between LDH levels and length of hospital stay, Spearman correlation coefficient showed no significant relationship (P-value= 0.253 and r= 0.15) (Figure 3).

Figure 3: Spearman’s correlation between LDH levels and length of hospital stay
Furthermore, LDH levels showed a significant and linear relation with leukocyte count, statistically (P-value= 0.017 and r= 0.262) (Figure 4).
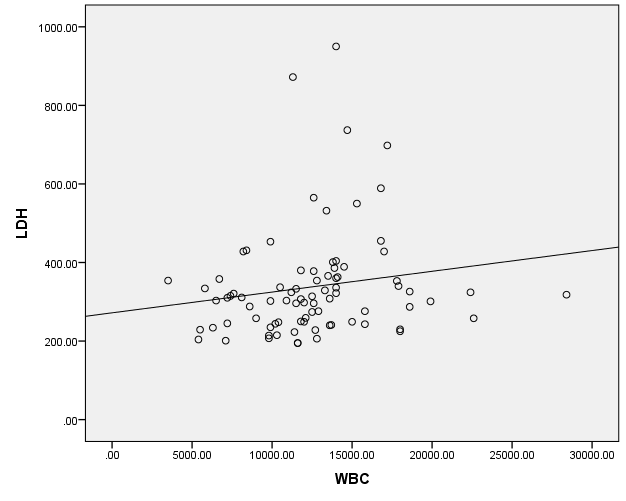
Figure 4: Spearman’s correlation between LDH levels and WBC count
Spearman correlation coefficient showed no significant relation among LDH and 1st hour ESR levels (P-value= 0.180 and r= -0.158) and LDH and 2nd hour ESR levels (P-value= 0.464 and r= -0.092) (Figure 5).

Figure 5: Spearman’s correlation between LDH level and ESR 2nd hour
Evaluation of CRP and LDH levels with Spearman correlation coefficient resulted in no significant relation, statistically (P-value= 0.673 and r= 0.05) (Figure 6).

Figure 6: Spearman’s correlation between LDH and CRP levels
DISCUSSION
In the present study, 279 consecutive patients who were hospitalized with the diagnosis of acute appendicitis, were evaluated. Pathology reports of 131 patients consisted of complicated appendicitis and 148 had simple appendicitis. Mean hospital stay in the complicated appendicitis group was 3.48 days and 3.03 days in the control group, and no significant difference was found. Furthermore, there was no statistically significant difference regarding clinical symptoms.
According to the results of a study done by Saldanha et al in 2015, LDH levels increased in association with disease progression [11]. In accordance, while we found no statistical difference between LDH levels of the two studied groups, the mean LDH plasma concentration in patients with complicated acute appendicitis was higher in comparison to patients with simple appendicitis. However, different results were achieved in another study done by Saldanha et al in 2019. Their results showed that even though levels of lipid peroxidation in pathological samples of inflammatory appendicitis were higher than samples attained from the normal appendix, LDH concentration was lower in inflammatory appendicitis samples [12].
In this study, we noted a statistically significant difference regarding the body temperature of patients of two groups (P-value= 0.05) and the mean body temperature of the complicated appendicitis group was 1 degree Celsius higher than the control group. In accordance, Eun Ko et al showed that higher body temperature degrees of the patients with acute appendicitis were statistically associated with perforation of the appendix [13].
Regarding laboratory results of WBC counts and neutrophil percentages, and 1st and 2nd hour ESR concentrations, we noted no statistical difference between the two groups. In contrast, Eun Ko et al. showed that ESR concentrations increased in association with the perforation of the appendix in a significant manner. In the same study, they discovered that WBC counts in the serum of patients with complicated appendicitis were not statistically different than patients with uncomplicated appendicitis; which is by our results [13]. Furthermore, Sengul and colleagues, reported significantly higher levels of WBC counts in complicated appendicitis patients in comparison to the uncomplicated appendicitis group [14].
Regarding the evaluation of CRP concentrations, we found a significant difference (P-value <0.0001) showing that patients with complicated appendicitis had higher levels of CRP in comparison to the uncomplicated appendicitis group. Similar results were achieved by Msolli and colleagues. According to their results, in comparison of CRP levels of patients with and without acute appendicitis, a statistically significant difference was noted and patients with acute appendicitis had higher CRP plasma concentrations [15]. Dal and colleagues reported similar results, as well [16]. Furthermore, Kim et al. showed that CRP increased significantly in patients with complicated appendicitis [17]. Ozan et al. reported high C-reactive protein level is a predictor for appendiceal perforation [18]. Shimoda et al. reported that high levels of CRP are associated with an increased risk of developing complications in appendicitis patients and conversion of surgery method from laparoscopic to open appendectomy [19]. Moon et al. showed that CRP above 7.05 mg/dL is associated with a high probability of complicated appendicitis, especially in young children or elderly patients who frequently present with vague symptoms [20].
Our study concluded that plasma concentration of LDH is not a reliable marker showing the probability of development of complications in acute appendicitis. On the other side, we found a significant relationship between plasma WBC levels and LDH concentrations, showing that higher counts of WBC were in association with higher levels of LDH. Although we noted no association regarding WBC and ESR levels and clinical symptoms with complicated appendicitis, there were significantly higher levels of CRP in patients with this condition.
In conclusion, we believe CRP concentrations are reliable markers showing an increased risk of developing complications in acute appendicitis patients.
AUTHORS' CONTRIBUTIONS
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Ozra Nouri and Peyman Virani. The first draft of the manuscript was written by Aisan Akhgari and Mahshid Dehghan and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
CONFLICTS OF INTEREST
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
REFERENCES
- Paulson EK, Kalady MF and Pappas TN.(2003). Clinical practice suspected appendicitis. N Engl J Med. 348(3):236-242.
- Bernard M, Jaffe H. (2005). Appendicitis. In: Brunicardi FC, Anderson D, Billiar T, Dunn D, Hunter J. Schwartz's principles of surgery, 8th Ed. New York, McGraw Hill, 1119-1139.
- Rezaee A, Ghaemee M, Motamed Alshariatee M, and Rashed T. (2004). Value measurement of serum CRP and WBC count in the diagnosis of patients with suspected acute appendicitis. J Gorgan Univ Med Sci, 6(13): 83-86.
- Abou-Nukta F, Bakhos C, Arroyo K, Young K, Jeremiah M, et al. (2006). Effects of delaying appendectomy for acute appendicitis for 12 to24 hours. Arch Surg. 141(5):504-506.
- Pruekprasert P, Maipang T, Geater A, Apakupakul N and Ksuntigij P. (2004). Accuracy in the diagnosis of acute appendicitis by comparing serum C-reactive protein measurements, Alvarado score, and clinical impression of surgeons. J Med Assoc Thailand. 87(3):296-303.
- Exp. Burd JF and Usategui-Gomez M. (1973). A colorimetric assay for serum lactate dehydrogenase. Clin Chim Acta 46(3):223–227.
- Kavakli HS, Erel O and Becel S. (2011). Oxidative stress in the diagnosis of acute appendicitis patients. Scientifi c Research and Essays. 6(8):1766-1770.
- Yilmaz FM, Yilmaz G, Erol MF, Koklu S and Yucel D. (2010). Nitric oxide, lipid peroxidation and total thiol levels in acute appendicitis. J Clin Lab Anal. 24(2): 63-66.
- Kaya M, Boleken ME, Kanmaz T, Erel O and Yucesan S. (2006). Total antioxidant capacity in children with acute appendicitis. Eur J Pediatr Surg. 16(1):34-38.
- Ozdogan M, Devay AO, Gurer A, Ersoy E, Devay SD, et al. (2006). Plasma total anti-oxidant capacity correlates inversely with the extent of acute appendicitis: a case control study. World J Emerg Surg. 1:6.
- Saldanha E, Ramachandrayya S A, Tauro L.F, Alva A, Alukal J, et al. (2015). Evaluation of antioxidant and cell death status in people with acute appendicitis: a preliminary study. Pak J Surg. 31(4), 227-231.
- Saldanha E, Tauro LF, Shivashankara AR, Alva A, Alukal J, et al. (2016). Correlation of histopathological observations of appendicitis tissue with glutathione, lipid peroxidation, and lactate dehydrogenase: An investigational study. Saudi Surg J. 4:71-76.
- Ryoung Eun Ko, Se Jin Park, and Ho Seung Kim. (2019). Relationship between the time required for transfer and outcomes in patients with appendicitis Experience at a tertiary military hospital in South Korea. Medicine (Baltimore). 98(43): e17715.
- Sengul S, Guler Y, Calis H, and Karabulut Z. (2020). The Role of Serum Laboratory Biomarkers for Complicated and Uncomplicated Appendicitis in Adolescents. J Coll Physicians Surg Pak. 30(4): 420–424.
- Msolli, M.A., Beltaief, K, Bouida, W, Nahla J, Mohamed Habib G, et al. (2018). Value of early change of serum C reactive protein combined to modified Alvarado score in the diagnosis of acute appendicitis. BMC Emerg Med. 18(1):15
- Dal F, Çiçek Y, Pekmezci S, Kocazeybek B, Bahartokman H, Konukoğlu D, et al. (2019). Role of Alvarado score and biological indicators of C-reactive protein, procalicitonin, and neopterin in diagnosis of acute appendicitis. Ulus Travma Acil Cerrahi Derg. 25(3):229-237.
- Kim M, Kim S. J, and Cho H. J. (2016). International normalized ratio and serum C-reactive protein are feasible markers to predict complicated appendicitis. World J Emerg Surg. 11: 31.
- Özozan, Ö. V and Vural, V. (2020). High C-reactive protein level as a predictor for appendiceal perforation. Ulus Travma Acil Cerrahi Derg. 26(1): 63-66.
- Shimoda M, Maruyama, T, Nishida K, Suzuki K, Tago T, et al. (2019). Preoperative high C-reactive protein level is associated with an increased likelihood for conversion from laparoscopic to open appendectomy in patients with acute appendicitis. Clin Exp Gastroenterol. 12: 141-147.
- Moon H M, Park B. S and Moon D. J. (2011). Diagnostic Value of C - reactive protein in Complicated Appendicitis. J Korean Soc Coloproctol. 27(3): 122–126.