Information Links
Related Conferences
Previous Issues Volume 9, Issue 1 - 2024
Retrospective Analysis of the Epidemiological Profile of Patients Submitted to Breast Reconstruction at a Public Hospital in the Northeast
Darley de Lima Ferreira Filho*, Nancy Cristina Ferraz de Lucena Ferreira, Thais de Lucena Ferreira
Barao of Lucena Hospital, Service of Breast Reconstruction, Recife, Pernambuco, Brazil
*Corresponding Author: Dr. Darley de Lima Ferreira Filho, Barao of Lucena Hospital, Service of Breast Reconstruction, Recife, Pernambuco, Brazil, Tel: 81999764602, Email: [email protected].
Received Date: January 23, 2024
Published Date: February 20, 2024
Citation: Filho DDLF, et al. (2024). Retrospective Analysis of the Epidemiological Profile of Patients Submitted to Breast Reconstruction at a Public Hospital in the Northeast. Mathews J Case Rep. 9(1):151.
Copyrights: Filho DDLF, et al. © (2024).
ABSTRACT
Introduction: Breast reconstruction is a right assured by the public health system to patients submitted to mastectomy. However, there are factors that delay the performance of this procedure. Objectives: To understand the epidemiological profile of women with breast cancer who underwent breast reconstruction in a reference hospital in the state of Pernambuco. Methods: This is an observational, retrospective research with an analytical character and descriptive approach. The data were collected through a questionnaire sociodemographic and clinical-surgical history of patients with breast carcinoma, and then analyzed by SPSS software, version 18 with the percentages of the categories evaluated by the Chi - square test, considering the significance level of 5%. The comparison of analyses was significant (p < 0.005), showing that the profile described is the most frequent in the group of patients evaluated. This search was submitted and approved by the Ethics and Research Committee on Human Beings of Fundação Amaury de Medeiros, CAAE: 42457420.1.0000.5193, Results: A non-probabilistic sample of 400 records was obtained in ten years at a tertiary hospital in Recife (PE), most of them with mean age between 46 and 59 years (45.3%), brown (61.1%), married (79.1%), with education until high school (60.7%), household professionals (45%), non-smokers (84.9%), who do not consume alcohol (94.9%) and had immediate reconstruction after mastectomy (70.3%). Conclusion: The findings support that patients with high educational levels are likely to undergo immediate breast reconstruction. Pointing out that the socioeconomic level significantly influences the rates of breast reconstruction after mastectomy.
Keywords: Breast Cancer Treatment, Epidemiology, Mastectomy, Breast Cancer, Breast Reconstruction.
INTRODUCTION
Breast cancer is a relevant public health problem, widely recognized as a disease that affects more frequently the female population over forty-five years of age, with the exception of non-melanoma skin cancer, being the main cause of death from cancer in women. women from all over the world, among women in high and low income countries [1,2]. There are some factors that are linked to the emergence of this condition, including the lifestyle adopted by sufferers [3-7].
There are several methods for treating breast cancer, this being a multidisciplinary treatment. Depending on the stage of the disease, local or systemic treatments can be used with more radical and conservative attitudes. In recent decades, surgical treatment has evolved from the more Haslted radical surgery for more conservative surgeries with immediate reconstruction [8,9]. Due to the aggressiveness of the procedure, a search was initiated for new, less aggressive techniques and ways to construct a new breast for women who suffered from multilating surgeries [10,11].
The accessibility of women who underwent breast reconstruction depends on the socio-demographic profile of these patients. It is also clear that underprivileged populations and educational levels have lower rates of breast reconstruction, which demonstrates lower availability and advice for immediate or delayed reconstruction [12,13].
In 2021, the Brazilian Society of Mastology published a note stating that, in the last decade, more than 110 thousand Brazilian women underwent mastectomy through the SUS, as part of the treatment for breast cancer. However, only 25 thousand underwent breast reconstruction, with an increase in absolute numbers being observed until 2014 with a slight reduction until 2017. In 2020, with the Covid-19 pandemic, there was an even more pronounced drop in the performance of these procedures, worsening a scenario that was already unfavorable [14].
It is clear that breast reconstruction and its evolution are related to several factors: economic, social and psychological, which contributed to delaying its acceptance for several decades [15-21]. Thus, the objective of our work is to understand the epidemiological profile, socioeconomic factors, clinical pathological characteristics and the relationship between immediate and delayed breast reconstruction in a reference public health network hospital in the State of Pernambuco, with the aim of understanding the association of these factors in the best way and change the lives of these women.
METHODOLOGY
It is an observational, retrospective study with an analytical character, with a descriptive approach. 400 patients diagnosed with breast cancer undergoing breast reconstruction admitted to the Mastology and Breast Reconstruction service at Hospital Barão de Lucena (HBL) in Recife-PE were evaluated.
For data analysis, a database was built in the Microsoft Excel spreadsheet, which was exported to the SPSS software, version 18, where the analysis was carried out. To evaluate the personal and clinical profile of the evaluated patients, percentage frequencies were calculated and respective frequency distributions were constructed.
To evaluate which factors influence the histological type and classification of TNM, contingency tables were constructed and the Chi-square test for independence was applied. In cases where the prerequisites for applying the Chi-square test were violated, the Fisher's Exact test was applied. In evaluating the relationship between the molecular subtype and the type of surgery and reconstruction, the Chi-square test was applied for homogeneity; as well as evaluating the distribution of the type of reconstruction according to the molecular subtype. All conclusions were drawn considering a significance level of 5%.
The project was submitted and approved by the Human Research Ethics Committee of the Amaury de Medeiros Foundation, CAAE: 35568920.0.0000.5191. Data collection began in September 2021, after approval by the ethics committee.
RESULTS
In table 1 we have the distribution of the socio-demographic profile of the patients evaluated. It can be seen that the majority of patients are from Recife (36.0%), are between 46 and 59 years old (45.3%), are brown (61.0%), married (79.3% ), studied until complete/incomplete high school (60.7%), works at home (45.0%), does not smoke (85.0%) and does not consume alcoholic beverages (95.0%).
Table 2 shows the distribution of the clinical profile of the patients evaluated. It was found that the majority of patients had a delay of more than 1 to 3 months of treatment (44.2%), ductal histological type (89.0%), TNM type II (51.0%), we performed a sectorectomy ( 57.7.3%), had immediate reconstruction performed in (70.3%), patients underwent CT (80.5%), radium (73.8%), and Luminal A molecular subtype (60.8 %).
Table 1. Distribution of the sociodemographic profile of the patients evaluated.
|
Evaluated factor |
N |
% |
p-valor |
|
Place of origin |
|
|
|
|
Capital |
145 |
36,1 |
0,221 |
|
Region Metropolitan |
117 |
29,3 |
|
|
Other region |
138 |
34,6 |
|
|
Age |
|
|
|
|
Until 30 age |
25 |
6,2 |
<0,001 |
|
31 a 45 age |
129 |
32,3 |
|
|
46 a 59 age |
181 |
45,3 |
|
|
60 age or more |
65 |
16,2 |
|
|
Color |
|
|
|
|
White |
136 |
33,9 |
<0,001 |
|
Brown |
245 |
61,1 |
|
|
Black |
29 |
5,0 |
|
|
Marital state |
|
|
|
|
Married |
325 |
79,1 |
<0,001 |
|
Single |
53 |
13,3 |
|
|
Widow |
13 |
2,8 |
|
|
Divorcide |
19 |
4,8 |
|
|
Level of education |
|
|
|
|
Without education |
6 |
1,2 |
<0,001 |
|
Education |
13 |
3,2 |
|
|
Fundamental Compl/incompl |
94 |
23,6 |
|
|
Médio Compl/incompl |
242 |
60,7 |
|
|
Superior Compl/incompl |
45 |
11,3 |
|
|
Profession |
|
|
|
|
Unemployed |
14 |
3,5 |
<0,001 |
|
Paid work |
167 |
41,8 |
|
|
Student |
15 |
3,8 |
|
|
Home |
180 |
45,0 |
|
|
Retiree |
24 |
6,0 |
|
|
SMOKE |
|
|
|
|
Yes |
62 |
15,1 |
<0,001 |
|
No |
338 |
84,9 |
|
|
Alcoolism |
|
|
|
|
Yes |
24 |
5,1 |
<0,001 |
|
No |
376 |
94,9 |
Table 2. Distribution of the clinical profile of the evaluated patients.
|
Factor avaliable |
N |
% |
|
Lag time |
|
|
|
Until 1 month |
148 |
36,8 |
|
More 1 to 3 months |
176 |
44,2 |
|
More 3 to 6 months |
62 |
15,5 |
|
More than 6 months to 1 year |
2 |
0,5 |
|
More 1 year |
12 |
3,0 |
|
Histological type |
|
|
|
Ductal |
356 |
89,0 |
|
Lobular |
15 |
3,7 |
|
Others |
29 |
7,3 |
|
TNM |
|
|
|
Level 0 |
25 |
6,2 |
|
Level I |
107 |
26,8 |
|
Level II |
204 |
51,0 |
|
Level III |
60 |
15,0 |
|
Level IV |
4 |
1,0 |
|
Type of surgery |
|
|
|
Mastectomy |
169 |
42,3 |
|
Quadrantectomy |
231 |
57,7 |
|
Time of reconstruction |
|
|
|
Imediate |
281 |
70,3 |
|
Late |
119 |
29,7 |
|
Chemotherapy |
|
|
|
Yes |
322 |
80,5 |
|
No |
78 |
19,5 |
|
Radiotheraphy |
|
|
|
Yes |
295 |
73,8 |
|
No |
105 |
26,2 |
|
Subtype molecular |
|
|
|
HER 2 |
34 |
8,4 |
|
Luminal A |
243 |
60,8 |
|
Luminal B |
65 |
16,3 |
|
Triple Negative |
58 |
14,5 |
Table 3. Distribuation of type reconstruction second the subtype molecular.
|
Type of reconstruction |
N |
% |
Subtype molecular |
|||
|
HER 2 |
Luminal A |
Luminal B |
TN |
|||
|
Mastectomy subcutaneous with implants |
36 |
9,0 |
5(14,7%) |
23(9,5%) |
4(6,2%) |
4(6,9%) |
|
Breast reconstruction with flap myocutaneos (GD) |
94 |
23,5 |
12(35,3%) |
54(22,2%) |
8(12,3%) |
20(34,5%) |
|
Flap with tissue autólogo: TRAM |
8 |
2,0 |
0(0,0%) |
7(2,9%) |
0(0,0%) |
1(1,7%) |
|
Reconstruction with Expander |
21 |
5,2 |
1(2,9%) |
14(5,8%) |
2(3,1%) |
4(6,9%) |
|
Lipofilling |
20 |
5,0 |
2(5,9%) |
12(4,9%) |
3(4,6%) |
3(5,2%) |
|
Reconstruction with implants |
41 |
10,3 |
0(0,0%) |
24(9,9%) |
12(18,5%) |
5(8,6%) |
|
Reconstruction oncoplastic with flap |
180 |
45,0 |
14(41,2%) |
109(44,9%) |
36(55,4%) |
21(36,2%) |
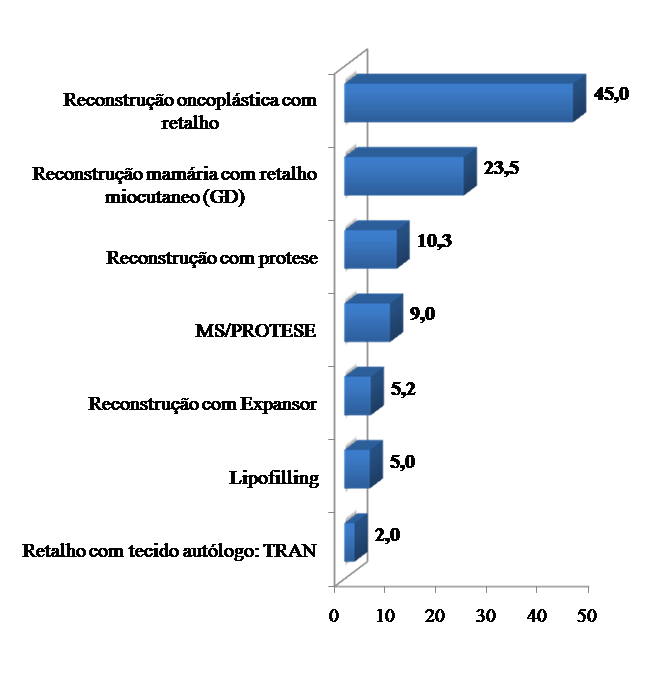
Figure 1.Distribution of patients according to type of reconstruction.
DISCUSSION
We observed that breast cancer has undergone major surgical evolution in recent years, from Halsted's mastectomy to conservative surgery and the advances in breast reconstruction that occurred in the 20th century. However, with the introduction of different oncoplasty techniques, women had a new option to improve the psychological trauma caused by the loss of the breast. Breast reconstruction surgery has been used on a large scale in the treatment of breast cancer, as it allows resections of large-volume tumors to achieve aesthetics and oncological results. Research has revealed that patients who choose breast reconstruction are motivated by body image for reasons of femininity and sexuality [22,23].
Our results from the socioeconomic, origin, educational and racial point of view, as well as age, marriage status, demonstrated in these patients that it did not have an influence on the use of breast reconstruction after conservative surgery or mastectomy, independent factors were considered for this type of procedure. Agarwal S et al found data similar to ours, together with Cristian CK in a study analyzing socioeconomic determinants in breast reconstruction [24,25]. The high level of patient satisfaction is associated with immediate reconstruction compared to mastectomy alone in psychosocial terms, sexual and physical [26,27].
The rate of patients who underwent immediate reconstruction was 70.3% and those who underwent delayed reconstruction was 29.7%. These data are positive when compared to literature data, in which 18.5% underwent immediate reconstruction while 9.5% underwent delayed reconstruction [28]. Morrow et al reported that approximately ¼ of their patients refused to undergo breast reconstruction after mastectomy, because they were afraid about the likelihood of interference with the detection of cancer recurrence [28-30].
Unlike the findings of Natalie et al, out of 866 patients, 768 did not undergo conservative surgery (88.7%) and 98 (11.3%) underwent oncoplasty surgery [31].
A Brazilian publication by Ruffo et al from 2017, on the trend of surgeries to treat breast cancer in Brazil, revealed that between January 2008 and December 2014, 193,596 surgeries were performed to treat breast cancer in the SUS, revealing a trend a reduction in the number of simple mastectomies with some stability in the numbers of BCS and radical mastectomies. In addition, there has been an increase in breast reconstructions using both implants and myocutaneous flaps. This study found a rate among patients who underwent mastectomy and reconstructive surgeries of 15% in 2008, with a significant increase in 2013 and 2014, which were 23.7% and 29.1%, respectively [32].
Another interesting fact, the majority of our patients were in clinical stage 0, I, II with 84% of patients, which allowed more conservative surgeries and immediate reconstruction than radical mastectomy. Wei Wu et al, in a survey of 47,123 in patients treated with mastectomy alone or mastectomy followed by breast reconstruction staging 0,I,II were 85%, similar to our findings. However, these data were not observed by Mansell et al. [33].
The most common histological type was Ductal and the majority of patients underwent mastectomy (43.0%). In the group of patients with the lobular histological type, the distribution of the type of surgery was homogeneous (33.3% for all types of surgery) and the time for immediate reconstruction was longer (73.3%). For other types of histological type, the majority underwent mastectomy (38.0%) and required immediate reconstruction (79.3%). The homogeneity test was not significant when comparing the distribution of the type of surgery and reconstruction time between the different histological types (p-value = 0.834 and 0.513, respectively), indicating that the distribution of the type and time of surgery is similar different histological types [34].
Regarding the molecular subtype of our patients, luminal A was the most found with 60% of cases, followed by luminal B in 16%, triple negative with 15% and HER-2 in 9%, these data are very similar by Wei Wu in the SEER survey in the United States National Cancer Institute program, where Luminal A was found in 68% of patients, with Her-2 in 6.1% and Triple negative in 13%. We observed that no difference was observed between the type of breast reconstruction with the different molecular subtypes. Patients with HER-2 and Triple negative molecular subtypes underwent less immediate breast reconstruction compared to luminal tumors, and also have a relatively higher risk of local recurrence [35].
The majority of our patients who underwent oncoplasty techniques used locoregional flaps (45%), breast implants and expanders (25%) in almost 70% of cases, leaving reconstruction with myocutaneous flaps with the large dorsal or Tram and fat grafting, for selected cases and later reconstructions. Offodile et al, in a retrospective study by the American College Of Surgeons, demonstrated that the most used reconstruction was with breast implant, and that reconstruction using flap and implant was rarer [2].
Regarding the level of education, it is clear that patients who underwent breast reconstruction had completed high school (60.7%), 11.3% had higher education. Therefore, it is noted that the higher the level of education of the patients, the greater the search for reconstruction, as in Albrecht [36].
Furthermore, it was noted that the majority of women who underwent breast reconstruction had some type of employment relationship. The study demonstrated that 41.8% of patients had some paid work. With this, we can infer that women in the job market seek more reconstruction procedures [37].
CONCLUSION
The findings support that patients with high educational levels are able to undergo immediate breast reconstruction. Also, the histological type of carcinoma and the molecular subtype did not interfere with breast reconstruction. We observed that the number of immediate breast reconstruction in patients with breast cancer had a significant increase.
REFERENCES
- American Cancer Society. (2020). Cancer Facts and Figures 2020. Atlanta: American Cancer Society.
- Browne JP, Jeevan R, Gulliver-Clarke C, Pereira J, Caddy CM, van der Meulen JHP. (2017). The association between complications and quality of life after mastectomy and breast reconstruction for breast cancer. Cancer. 123(18):3460-3467.
- Siegel R, Ma J, Zou Z, Jemal A. (2014). Cancer statistics, 2014. CA Cancer J Clin. 64(1):9-29.
- WHO. Health statistics and information systems 2018. World Health Organization. Available at: http://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.html
- Hutchinson J, Burley VJ, Greenwood DC, Thomas JD, Cade JE. (2011). High-dose vitamin C supplement use is associated with self-reported histories of breast cancer and other illnesses in the UK Women's Cohort Study. Public Health Nutr. 14(5):768-777.
- Cabral ALLV, Giatti L, Casale C, Cherchiglia ML. (2019). Vulnerabilidade social e câncer de mama:diferenciais no intervalo entre diagnóstico e o tratamento em mulheres de diferentes perfis sociodemograficos. Ciência e Saúde Coletiva, Rio de Janeiro. 24(2):613-622.
- Costa LLN, Sardinha AHL, Verzaro PM, Lisboa LLC. (2019). Mortalidade por Câncer de Mama e Condições do desenvolvimento Humano no Brasil. Revista Brasileira de Cancerologia. 65(1):99-104.
- Morrow M, Jagsi R, Alderman AK, Griggs JJ, Hawley ST, Hamilton AS, et al. (2009). Surgeon recommendations and receipt of mastectomy for treatment of breast cancer. JAMA. 302(14):1551-1556.
- Coelho GVBF, Nogueira FDVM, Vagner Franco da Silveira Jr, Andrade CZND, Carrara HHA, Oliveira HFD, et al. (2014). Avaliação oncológica após reconstrução mamária com lipoenxertia: subtítulo do artigo. Revista Brasileira de Cirurgia Plástica, São Paulo. 29(2):243-247.
- Champaneria MC, Wong WW, Hill ME, Gupta SC. (2012). The evolution of breast reconstruction: a historical perspective. World J Surg. 36(4):730-742.
- Badr H, Acitelli LK, Taylor CL. (2008). Does talking about their relationship affect couples' marital and psychological adjustment to lung cancer? J Cancer Surviv. 2(1):53-64.
- de Almeida RJ, de Moraes Luizaga CT, Eluf-Neto J, de Carvalho Nunes HR, Pessoa EC, Murta-Nascimento C. (2022). Impact of educational level and travel burden on breast cancer stage at diagnosis in the state of Sao Paulo, Brazil. Sci Rep. 12(1):8357.
- Martin-Pandura I, Gregato G, Marighetti P, Mancuso P, Calleri A, Corsini C, et al. (2012). The white adipose tissue used in lipotransfer procedures is a rich reservoir of CD34 progenitors able to promote câncer progression. Cancer Res. 72(1):325-334.
- Sociedade Brasileira de Mastologia. (2021). Cai número de cirurgias de reconstrução mamária no SUS durante a pandemia. [Internet]. Rio de Janeiro (RJ). Available at: https://www.sbmastologia.com.br/cai-numero-de-cirurgias-de-reconstrucao-mamaria-no-sus-durante-a-pandemia/
- Hassan H. (2020). Human Breast Milk Bank: A Valuable Issue for Working Mothers. American Research Journal of Public Health. 3(1):1-3.
- Hassan H. (2011). Impact of Nursing Intervention on Relief of Breast Engorgement: Among Women with Caesarean Section. A Thesis Submitted to Faculty of Nursing, Benha University, Egypt.
- Hassan H, ELKholy G, Ateya A, Hassan A. (2020). Breast Engorgement among Women with Caesarean Section: Impact of Nursing Intervention. Education, Society and Human Studies. 1(2):22-55.
- Zagloul M, Naser El, Hassan H. (2020). Influence of Hot Compresses Versus Cabbage Leaves on Engorged Breast in Early Puerperium. International Journal of Studies in Nursing. 5(2):7-14.
- Hassan H, EL-Kholy G, Ateya A, Hassan A. (2020). Breast Feeding Knowledge and Practices among Primiparous Women with Caesarean Section: Impact on Breast Engorgement in Upper Egypt. Communication, Society and Media. 3(2):34-78.
- Hassan H, Gamel W, Hassanine Sh, Sheha E. (2020). Fenugreek Seed Poultice versus Cold Cabbage Leaves Compresses for Relieving Breast Engorgement: An interventional Comparative Study. Journal of Nursing Education and Practice. 10(5):82-99.
- Abd-Allah N, Nasr E, Hassan H. (2017). Impact of a Breast Feeding Educational Program for Mothers Having Pre-Term Infants in General Hospitals in Port Said. International Journal of Novel Research in Healthcare and Nursing. 4(3):215-225.
- Nunes BAP, Siqueira SL, Pereira SM, Pacheco TJ, Pessanha TDO, Mendonça SB. (2012). Perfil epidemiológico dos pacientes diagnosticados com câncer de mama em Campos dos Goytacazes (RJ), Brasil. Rev Bras Mastologia. 22(4):117-123. Available at: https://www.mastology.org/wp-content/uploads/2015/06/MAS_v22n4_117-123.pdf
- Duggal CS, Metcalfe D, Sackeyfio R, Carlson GW, Losken A. (2013). Patient motivations for choosing post mastectomy breast reconstruction. Ann Plast Surg. 70(5):574-580.
- Clough KB, Benyahi D, Nos C, Charles C, Sarfati I. (2015). Oncoplastic surgery: pushing the limits of breast-conserving surgery. Breast J. 21(2):140-146.
- Clough KB, Meredith I. (2019). The oncoplastic frenzy: beware the swing of the pendulum. Ann Surg Oncol. 26(12):3792-3793.
- Eltahir Y, Werners LLCH, Dreise MM, Van Emmichoven IAZ, Jansen L, Werker PMN, et al. (2013). Quality-of-life outcomes between mastectomy alone and breast reconstruction: comparison of patient-reported BREAST-q and other health-related quality-of-life measures. Plast Reconstr Surg. 132(2):201e-209e.
- Atisha DM, Rushing CN, Samsa GP, Locklear TD, Cox CE, Shelley Hwang E, et al. (2015). A national snapshot of satisfaction with breast cancer procedures. Ann Surg Oncol. 22(2):361-369.
- Losken A, Hart AM, Chatterjee A. (2017). Updated Evidence on the Oncoplastic Approach to Breast Conservation Therapy. Plast Reconstr Surg. 140(5S Advances in Breast Reconstruction):14S-22S.
- Clough KB, Van la Parra RFD, Thygesen HH, Levy E, Russ E, Halabi NM, et al. (2018). Long term results after oncoplastic surgery for Breast Cancer: 10 year follow up. Ann Surg. 268(1):165-171.
- Morrow M, Li Y, Alderman AK, Jagsi R, Hamilton AS, Graff JJ, et al. (2014). Access to breast reconstruction after mastectomy and patient perspectives on reconstruction decision making. JAMA Surg. 149(10):1015-1021.
- Almeida NR, Brenelli FP, Dos Santos CC, Torresan RZ, Shinzato JY, Cardoso-Filho C, et al. (2021). Comparative study of surgical and oncological outcomes in oncoplastic versus non oncoplastic breast-conserving surgery for breast cancer treatment. JPRAS Open. 29:184-194.
- Freitas-Júnior R, Gagliato D, Moura Filho J, Gouveia P, Rahal R, Paulinelli R, et al. (2017). Trends in breast cancer surgery at Brazil’s public health system. J Surg Oncol. 115(5):544‐549.
- Mansell J, Weiler-Mithoff E, Martin J, Khan A, Stallard S, Doughty JC, et al. (2015). How to compare the oncological safety of oncoplastic breast conservation surgery - To wide local excision or mastectomy? Breast. 24(4):497-501.
- Ferreira DLF, Ferreira NCFL, Abreu e Lima MC, Ferraz AAB, Martins DBG, Ferreira TL. (2017). Invasive triple negative breast cancer basal and non- basal like Immunophenotypes: Prognostic Implications. Mastology. 27(4)276-286.
- Wu W, Cheng S, Deng H, Wu J, Mao K, Cao M. (2016). Impact of Breast Cancer Subtype Defined by Immunohistochemistry Hormone Receptor and HER2 Status on the Incidence of Immediate Postmastectomy Reconstruction. Medicine (Baltimore). 95(3):e2547.
- Offodile AC, Tsai TC, Wenger JB, Guo L. (2015). Racial disparities in the type of postmastectomy reconstruction chosen. J Surg Res. 195(1):368-376.
- Sandberg JC, Strom C, Arcury TA. (2014). Strategies used by breast cancer survivors to address work-related limitations during and after treatment. Womens Health Issues. 24(2):e197-e204.