Previous Issues Volume 1, Issue 2 - 2016
Nonketotic Diabetic Hemichorea-Hemiballismus in the Emergency Department
Alan Lucerna, James Espinosa*
Department of Emergency Medicine, Rowan University SOM Kennedy University Hospital, Stratford, NJ, USA
Corresponding Author: James Espinosa, Department of Emergency Medicine, Rowan University SOM Kennedy University Hospital, 18 East Laurel Road, Stratford, NJ 08084, USA, Tel: +1 646 241 5695; E-Mail: [email protected]
Received Date: 14 Mar 2016
Accepted Date: 04 Apr 2016
Published Date: 21 Apr 2016
Copyright © 2016 Espinosa
Citation: Lucerna A and Espinosa J. (2016). Nonketotic Diabetic Hemichorea-Hemiballismus in the Emergency Department. Mathews J Emergency Med. 1(2): 009.
ABSTRACT
We present a case of a 59-year old diabetic Jamaican male who presented to the emergency department with hemichorea- hemiballismus (HC-HB). HC-HB is a rare presentation of nonketotic hyperglycemia. While previously described in radiology, neurology and endocrinology literature, reports of this hyperkinetic movement caused by hyperglycemia are rare in the emergency medicine literature. Various conditions may cause hemichorea-hemiballismus. We highlight a case that illustrates the important distinguishing features of nonketotic hyperglycemic hemichorea-hemiballismus diagnosed in the emergency department.
KEYWORDS
Nonketotic Diabetic Hemichorea-hemiballismus; Hemichorea-hemiballismus; Emergency Department and Nonketotic Diabetic Hemichorea-hemiballismus; Nonketotic Hyperglycemia Presentations.
INTRODUCTION
Hemichorea-hemiballismus (HC-HB) is a rare presentation of nonketotic hyperglycemia. Chorea is characterized by involuntary, poorly patterned, short lasting jerky movements [1,2]. Ballismus, on the other hand, is described as large amplitude flailing movements [2]. While previously described in journals of radiology, neurology and endocrinology literature, reports of this hyperkinetic movement caused by hyperglycemia are rare in the emergency medicine literature. While various conditions may cause hemichorea-hemiballismus, we present a case that illustrates the important distinguishing features of nonketotic hyperglycemic hemichorea-hemiballismus.
CASE PRESENTATION
A 59-year-old Jamaican male presented to the emergency department (ED) with complaints of involuntary movements of his left upper and left lower extremities that started one day prior to arrival. The patient's family also reported an episode of transient slurred speech at the onset of the patient's sympA 59-year-old Jamaican male presented to the emergency department (ED) with complaints of involuntary movements of his left upper and left lower extremities that started one day prior to arrival. The patient's family also reported an episode of transient slurred speech at the onset of the patient's symptoms which resolved prior to arrival to the ED. The patient denied any other neurological complaints. The patient had no history of seizures and denied any history of drug or alcohol use. He had no recent travel, trauma, illness or hospitalization. His only medical history was diabetes. He admitted that he had not taken his prescribed metformin and glyburide for several weeks. He did not have health insurance coverage and stated that he had not been able to afford his medications and glucose test strips. The patient's physical exam showed a very lean man in no acute distress. There were no cranial nerve deficits and no facial asymmetry. He had no visual field cuts. His extremities were noted to have normal strength and sensation. His gait was steady and no ataxia was observed. He was noted to have irregular, short-lasting, involuntary movements of his left upper and left lower extremities during the exam. Laboratory findings include a finger stick glucose that was over 500 mg/dL. Serum basic metabolic panel revealed the following abnormalities: Glucose: 591 mg/dL, sodium: 132 mm/L, and a creatinine of 1.35 mg/dL. The remaining values were within normal limits and there was no anion gap. The urine drug screen was unremarkable and his ECG did not show any ischemic changes. A CT scan was obtained and showed a unilateral hyper attenuation of the caudate nucleus and lenti form nucleus on the right (Figure 1). An insulin drip and IV fluids were initiated in order to correct the hyperglycemia and kidney injury. After consulting with the neurology service, the patient was admitted overnight to the intensive care unit. Neurology recommended the consideration of focal seizures. A dose of lorazepam was administered in the emergency department.
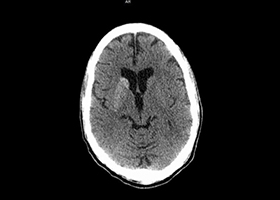
Figure 1: CT scan of the brain without contrast showing a unilateral hyper attenuation of the caudate nucleus and lenti form nucleus on the right.
After being on the insulin drip overnight, glycemic control was achieved and the patient's involuntary movement resolved completely. The patient's HgbA1c was 17.8%. A follow up MRI of the brain showed that the right caudate nucleus and the right lentiform echoes were increased in the T1 weighted signal corresponding to the same areas of increased attenuation reported on the CT scan of the brain (Figure 2).
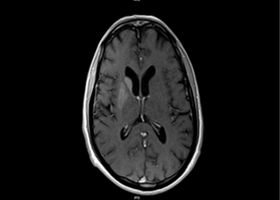
Figure 2: MRI of brain. Right caudate nucleus and right lenti form echoes increased in the T1 weighted signal. Corresponds to areas of increased attenuation in CT in Figure 1.
The patient's symptoms did not recur during his hospital stay. After being seen by the neurologist and endocrinologist, the patient was discharged home on insulin therapy.
DISCUSSION
Initially reported in 1960, diabetes has since been reported worldwide as a rare cause of hemichorea-hemiballismus [1,3]. The majority of the reports have been attributed to non-ketotic hyperglycemic type 2 diabetes. However, abnormal movements have also been reported with ketotic hyperglycemic type 1 patients [2, 3]. The chorea and ballismus can be unilateral or bilateral [5]. Various disease entities other than diabetes can cause hemichorea- hemiballismus. Focal lesions from ischemic or hemorrhagic strokes should be considered, since most presentations of HC-HB caused by hyperglycemia occur mostly in patients over 60 years old [1]. Drugs, infections, seizures, neurodegenerative disorders, and neoplasms should be also considered, as well systemic etiologies like thyrotoxicosis, Wilson's disease and systemic lupus erythematosus [2-4]. In patients with recent illness from Strep pharyngitis, Syndenham's chorea secondary to a post-streptococcal neurological disease should also be entertained in the differential diagnosis [4]. Several competing mechanisms have been proposed to explain the pathophysiology of hyperglycemic chorea-ballismus. The exact mechanism however, has not been clearly delineated. In nonketotic hyperglycemia, cerebral metabolism is shifted from the aerobic Krebs cycle to anaerobic pathways. The brain's shift energy results in the limited availability of both acetylcholine and gamma-aminobutyric acid (GABA) in the basal ganglia. Coupled with metabolic acidosis and lack of energy production, the overall effect on the basal ganglia has been proposed to clinically cause chorea [7]. Additional possible mechanisms include cerebral vascular insufficiency, local micro-infarction and micro-hemorrhage, hyperviscosity, and infection [3,4]. As noted, our patient demonstrated an abnormal CT scan of the brain on presentation. However, the CT scan can initially be normal, with the subsequent development of the finding of subtle hyperdensity in striatal region. The modality of choice for assessing suspected nonketotic hyperglycemic hemichorea- hemiballismus is a magnetic resonance imaging (MRI) scan of the brain. Typically, signal changes are demonstrated in the caudate nucleus and/or putamen. These findings are contralateral to the symptomatic side. T2/fluid attenuation inversion recovery (FLAIR) images will show hypointense areas while on diffusion weighted images (DWI) restricted diffusion can be seen. The most consistent finding of the disease however is the hyperintensity in the putamen and/or caudate on T1 weighted image sequences [5]. Attempts to explain these radiographic findings have been subject of debate. One hypothesis suggests that the T1 hyperintensity is due to swollen reactive astrocytes, also called gemistocytes. Evidence to support this came from biopsy of the hyperintense putaminal lesion demonstrating abundant reactive astrocytes. Alternatively, is has been suggested that the signal abnormality represents putaminal petechial hemorrhages. Another theory is that demyelination- -similar to that seen in diabetic peripheral neuropathy--leads to water exchange between the myelin and the axon with resultant T1 shortening. Some authors have also speculated that there could be localized Wallerian degeneration reflecting transient ischemic changes or desiccation [7]. While our patient was male and of Jamaican decent, a majority of the cases described involve Asian women in their early seventies [1,7]. Recently, however, the diagnosis has been reported in patients as young as 17 years of age. [3,4]. Choreaballismus, whether unilateral or bilateral could be the initial presentation of diabetes or can be due to poor glycemic control in a known diabetic. The cornerstone the treatment is aggressive glucose management. Resolution of hemichorea-hemiballismus coincides with the reduction of the glucose in the majority of the cases [1-5]. Benzodiazepine treatment has also been discussed in the literature. In addition to benzodiazepines, neuroleptic drugs can also be used and have found to be effective in some refractory cases [1,3]. While the patient may show resolution of clinical symptoms, the characteristic findings on imaging studies may persist for months [1].
CONCLUSION
In conclusion, nonketotic hyperglycemic hemichorea-hemiballismus is an interesting and important differential diagnosis in patients presenting to the emergency department. With prompt recognition and treatment of the underlying metabolic disorder, hemichorea-hemiballismus is highly treatable with an overall excellent prognosis.
REFERENCES
- Padmanabhan S, Zagami AS, Ann M and Poynten AM. (2013). A Case of Hemichorea-Hemiballismus Due to Nonketotic Hyperglycemia. Diabetes Care. 36(4), e55-e56.
- Yasuhara A, Wada J and Makino H. (2008). Bilateral dystonia in type 1 diabetes: a case report. Journal of Medical Case Reports. 18(2), 352.
- Abdelghany M and Massoud S. (2014). Nonketotic Hyperglycemic Chorea. Case Reports in Neurological Medicine. 2014(2014), Article ID 128037, 3.
- Khan I, Kant C, Sanwaria A and Goyal A. (2012). Hemichorea- hemiballismus as the presenting manifestation of nonketotic hyperglycemia in an adolescent with undiagnosed type 2 diabetes mellitus. Letters to the Editor. Indian Journal of Endocrinology and Metabolism. 16(Supplement 1), S129-S131.
- Knipe H, Gaillard F et. al. Non-ketotic hyperglycaemic hemichorea.
- Bizet, J, Cooper CJ, Quash R, Rodriguez E, et al. (2014). Chorea, Hyperglycemia, Basal Ganglia Syndrome (C-H-BG) in an uncontrolled diabetic patient with normal glucose levels on presentation. American Journal of Case Reports. 15, 143-146.
- Hansford BG, Albert D and Yang E. (2013). Classic neuroimaging findings of nonketotic hyperglycemia on computed tomography and magnetic resonance imaging with absence of typical movement disorder symptoms (hemichorea-hemiballism). J Radiol Case Reports. 7(8), 1-9.