Previous Issues Volume 1, Issue 1 - 2016
Laparoscopic Colostomy in ASA: An Advanced Rectum Cancer Option
Morelos Adolfo Garcia Sanchez1,Mireya De La Fuente Gonzalez2 ,Alvaro Tomas Ruz Concha3,Jimenez Muñoz Sergio Alejandro2,Santillán Cisneros Gustavo Armando2 , Rosales De La Cruz Jose Gilberto2
Corresponding Author: Morelos Adolfo Garcia Sanchez, General Practitioner and Colonic and Rectal Surgeon at Dr. Gaudencio Gonzalez Garza General Hospital Specialized Medical Unit, La Raza National Medical Cente, Mexico, Tel: 01 (52) 5524-5900; Email: [email protected] Received Date: 21 Jul 2016 Accepted Date: 30 Aug 2016 Published Date: 01 Sep 2016 Copyright ©2016 Garcia SMA Citation: Garcia SMA, De La Fuente GM, Ruz CAT, Jimenez MSA, et al. (2016). Laparoscopic Colostomy in ASA: An Advanced Rectum Cancer Option.Mathews J Gastroenterol Hepatol 1(1): 003. ABSTRACT
Introduction:The first description of a laparoscopic colon was in the year 1990. The advantages are a postoperative analgesic dose reduction, also a better immune and inflammatory response, besides a shorter recovery time and hospital discharge with a superior esthetic. Objectives:To describe our experience about mortality, morbidity and / or effectiveness of technical and clinical success, associated with the surgical laparoscopic in patients who have suffered from stoma, in the Department of Surgery of Colon and rectum. Methods:Descriptive, observational, retrospective and cross-sectional study; with central tendency measures. Describing patients treated with laparoscopic colostomy derivative, the May 2012 to October 2015. Results:17 patients were diagnosed with rectum cancer in clinical stage IV with the only indication of laparoscopic colostomy of this study; describing the hereditary cancer and clinical background which was 70% of all these cases; delivering a result of 2% morbidity and 0% mortality. Conclusions:The surgical technique: Laparoscopic colostomy in asa (LCA), with outstanding results obtained from this study in the hospital; it has proved to be a quick, simple, effective, feasible and safe surgical method which nowadays has become unique. KEYWORDS
Resection; Ileus; Laparoscopic; Stoma; Colostomy. INTRODUCTION
Innovation laparoscopy started in 1902 by German doctor Kelling performing laparoscopic pneumoperitoneum exploration applied to a canine [1]. It was not until 1983 that the first laparoscopic appendectomy is awarded by Semm [2]. In 1985 Dr. Erich Muhe makes the first laparoscopic cholecystectomy, historical fact disputed and lost by the French surgeon Phillipe Mouret in 1987 [3]. In recent decades, laparoscopic surgery has been gaining place, and the opportunity to develop and be applied in most diseases or surgical pathologies; becoming the gold standard in cholecystitis, gastroesophageal reflux disease and morbid obesity [1]. Moses Jacobs introduced laparoscopic colectomy for the treatment of colorectal cancer and benign pathologies. The first description of a laparoscopic colon resection is reported in the year 1990 [4-6]. In consequence a race began for descriptions of laparoscopic surgeries assisted since 1991, regarding to colorectal diseases [7]. There are advantages of laparoscopic surgery of the colon and rectum, regarding to the open one; such as a dose reduction in postoperative analgesic [8]. The Best immune and inflammatory response after surgery, a big recovery time reduction and hospital discharge with a superior cosmetic result [9, 10]. We can add other advantages: less postoperative ileus, less intraoperative bleeding, early oral tolerance, low pulmonary complication rate as well as a quick surgical wound healing [11, 12]. It also presents a lower incidence of postoperative adhesions at the same time decreasing the frequency of reoperations because of the intestinal occlusion [13]. Talking about the disadvantages we can describe many situation as the following: technical complexity, cost of instruments, the need for adequate learning curve, uncertainty on the radicality in oncologic resection, the inability to mobilize large organ (surgical specimen) and a prolonged surgical time [14-16]. Our objective is to describe our experience in mortality, morbidity, clinical efficacy and surgical technique for palliative treatment in patients with unresectable rectal cancer or regionally advanced, with the surgical approach of laparoscopic colostomy in asa (LCA) in the last 3 years in the Surgery of Colon and Rectal service. METHODS
Descriptive, observational, retrospective and cross-sectional study; conducting a review of clinical records diagnosed with an inoperable rectal cancer loco regionally advanced with or without metastases and / or adhesions; which are treated with LCA at the General Hospital “Dr. Gaudencio González Garza “of the Medical Unit of High Specialty of the National Medical Center “ La Raza “, of the “Instituto Mexicano del Seguro Social”, during the period from May 2012 to October 2015. It was obtained from each patient record: sex, age, chronic degenerative medical history, surgical and oncology; specific clinical diagnosed with rectal cancer occlusive or with an approaching of occlusive, operative time, operative bleeding, hospital stay, local and general complications. Conversion to open surgery, via oral begin, overall morbidity and mortality. All patients met the criteria with the pre surgical protocol consisted of: Medical history with a physical examination completed. General laboratories which included carcinoembryonic antigen and alpha fetoprotein, chest radiography, computed tomography (CT) scans, liver ultrasound, colonoscopy (partial to biopsy, intraoperative or postoperative seeking synchronous or another hereditary syndrome); finally, histologic confirmation of “Rectum Adenocarcinoma”. LCA is projected with a prior review of the stoma, patient’s informed consent, once patients were discharged from hospital they were observed during 21 days, removing surgical sutures and the conduit used in the patients. With referral to Oncology to keep handling with neoadyudancia (a likely option for curative resection post) and / or palliative.
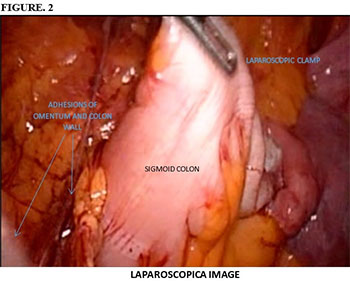
LCA surgical technique exposed in this manuscript is original and never described before in the literature, being described as follow: In the operating room under prior general aseptic and anesthesia in patient's supine. A veress needle is used with pneumoperitoneum around 12 mm of mercury, placing a 12 mm trocar at umbilical level, then a camera of 30 degrees is introduced into the body allowing us an exploration of the abdominal cavity systematised Figure 1, A second trocar 12 mm under direct vision is placed at the level of the future premarked colostomy, the colonic segment intended colostomy is located and it moves with a traumatic gripping clamp to confirm that may rise at the level of the abdominal wall Figure 2. Otherwise you can dissect adhesions allowing a better mobilization of the colon. Colonic segment chosen is externalized focusing on the perimeter of the trocar, removing it and placing a conduit in the anti-mesenteric handle edge, adjusting the orifice of the stoma and accomplishing pneumoperitoneum again. It is reviewed there is no tension or torsion. The umbilical trocar and the pneumoperitoneum are removed with the usual closure. The stoma is sutured and separated with 00 prolene from the colon to the skin Figure 3. Without any attachment to the aponeurosis.


RESULTS
In this period 17 patients were assited with rectal cancer diagnosis (100% of cases) with clinical stage IV; with intestinal occlusion: 4 urgent (real) and 13 priority (felt); All patients underwent sigmoid colon LCA. Of which 10 (60%) were males and 7 (40%) were females, with an average of 43 years and a range of 20-70 years. Only 7 (40%) of the diseases were associated as the following: - Diabetes Mellitus 2 : 3 patients. - Arterial hypertension : 2 patients - Asthma : 1 patients - Ischemic heart disease : 1 patient.
Twelve patients had a history of hereditary colon cancer, symbolizing 70%, three patients 18% only with a history of other cancer which is not colon cancer (breast, thyroid and cervical) and the two remaining patients they represented 12% without a history of cancer.
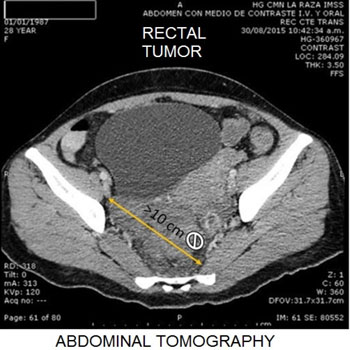
Six patients had less surgical history: two appendectomy patients, one anal fissure patient, another one because of the hemorrhoidectomy, also a caesarean one and last but not least a sigmoid colon volvulus case. Seventeen patients of the study were arbitrarily classified according to their tumor size by CT Figure 4 more or less than 10 cm in diameter, being associated their clinical history in each case; in patient's 100% constipation was presented, 94% was abdominal distension, fifteen patients (88%) presented anemia, weight loss being the same 88% and rectal bleeding 82%, the actual intestinal occlusion and fever in four cases representing 24% of these being the same. Patients did not present intermittent diarrhea neither overflow evacuation nor pain. In summary, the patient's clinical characteristics relationship because of the tumor size are presented in Table 1.
Table 1: clinical characteristics of patiens by tumorsize.
| CLINICAL MANIFESTATION | TT*>10CM=7TOTAL | TT*< 10CM=7 TOTAL | ||
|---|---|---|---|---|
| MENS | WOMEN | MENS | WOMEN | |
| ANEMIA | 3 | 2 | 6 | 4 |
| FEVER | 0 | 0 | 3 | 1 |
| CONSTIPATION | 4 | 3 | 6 | 4 |
| INTESTINAL OCCLUSION | 0 | 0 | 3 | 1 |
| HYPOREXIA | 2 | 1 | 4 | 3 |
| ASTHENIA AND ADINAMIA | 2 | 1 | 3 | 3 |
| WEIGHTLOSS | 3 | 2 | 6 | 4 |
| ABDOMINAL PAIN | 2 | 1 | 6 | 4 |
| TRANSRECTAL BLEEDING | 3 | 1 | 6 | 4 |
| ABDOMINAL DISTENSION | 3 | 3 | 6 | 4 |
* TT. TUMOR SIZE.
Table 2 the specific results of the surgical approach LCA are evaluated. There was no conversion to open surgery. Adherenciolisis was performed in seven patients representing 40% (without the need to place another port and / or trocar). Eight patients were found with metastases representing 47% of the group.
The average operating time was 33 minutes with a range from 23 to 50 minutes, and as mode 30 minutes. Regarding to bleeding during surgery it had an average of 35 milliliters with a range from 20 to 100 milliliters. There were no reported local complications and general or systemic complications only one patient suffered from pneumonia but had an adequate response to treatment. The days of hospital stay was 4 days in average with a range from 3 to 9 days. And finally according to tumor indicators we found that only eight patients had elevated carcinoembryonic antigen being 47%, and three elevated alpha-fetoproteins which are 18% of the study group. The begin of via oral method was immediately within the first 12 hours in all patients. Morbidity was less than 2% and no mortality.
Table 2: clinical characteristics of patiens by tumorsize.
| AGE/SEX | CONVERSION TO OPEN SURGERY | ADHESIONS | METS1 | TIME SURGICAL MINUTES | SURGICAL BLEEDING ML | COMPLICATIONS | DHS2 | CEA3/AFP4 | INTESTINAL OCCLUSION | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| LOCAL | GENERAL | URGENT | PRIORITY | ||||||||
| 20/H | NO | YES | NO | 23 | 25 | NO | NO | 4 | 35/2 | X | |
| 26/H | NO | NO | NO | 35 | 20 | NO | NO | 4 | 3/2 | X | |
| 27/M | NO | YES | NO | 28 | 40 | NO | NO | 3 | 18/3 | X | |
| 29/M | NO | NO | YES | 27 | 30 | NO | NO | 4 | 87/32 | X | |
| 29/H | NO | NO | NO | 32 | 20 | NO | NO | 3 | 4/2 | X | |
| 31/M | NO | YES | NO | 30 | 40 | NO | NO | 4 | 3/1 | X | |
| 34/H | NO | YES | NO | 35 | 50 | NO | NO | 4 | 44/2 | X | |
| 40/M | NO | YES | NO | 30 | 20 | NO | NO | 3 | 6/3 | X | |
| 43/H | NO | NO | SI | 35 | 50 | NO | NO | 4 | 4/2 | X | |
| 46/M | NO | YES | YES | 40 | 30 | NO | NO | 5 | 115/9 | X | |
| 48/H | NO | NO | NO | 25 | 20 | NO | NO | 3 | 3/2 | X | |
| 52/M | NO | YES | YES | 40 | 40 | NO | NO | 4 | 2/4 | X | |
| 53/H | NO | NO | YES | 50 | 100 | NO | NO | 4 | 35/90 | X | |
| 58/H | NO | NO | YES | 30 | 30 | NO | NO | 5 | 47/2 | X | |
| 65/H | NO | NO | NO | 25 | 40 | NO | NO | 4 | 4/3 | X | |
| 67/H | NO | NO | YES | 45 | 30 | NO | NO | 4 | 59/2 | X | |
| M | NO | YES | NO | 30 | 20 | NO | YES | 9 | 4/4 | X | |
1METS: METASTASIS 2DHS: DAYS OF HOSPITALS STAY 3CEA: CARCINOEMBRYONIC ANTIGEN 4AFP: ALFAFETO PROTEIN
DISCUSSION
These patients we published are unfortunately suffering from a terminal pathology, unresectable advanced rectal cancer and / or with a fatal prognosis in the short term; They are offered palliative treatment or an opportunity for neoadyudancia, and thus hope for a cure, with a temporary stoma laparoscopic surgical; being quick, effective and simple processing [17]. Our data show that the LCA technique is feasible, safe and reproducible. As the experience reported in other series, although with some variations in surgical technique, however, with this technique done we were able to short the surgical time and bleeding up to 50% without placing a third trocar [18-20]. With excellent results without having to create a confused evastatingly complex procedure and, conversely, is achieved simplifies the most; with only a report almost similar in all the literature [21, 22]. It is important to rule out that unlike the rest of the published series is not necessary to place the third port or more of them [23]. We only applied two, one at the site will be occupied by the colostomy and the second that is the camera, that's why the genius and originality of this technique.
Recently, the minimally invasive management (laparoscopic) has gained a better conventional place, and have already been reported colorectal surgeries by the socalled unique port, further improving the surgical management of these diseases [24-26].
The LCA is a simple surgical technique, and aims to be easily reproducible with no morbidity and no mortality. It is essential to note that grants benefits to cancer patients immeasurably, thus achieving a quick postoperative recovery without complicomplications, with a better and prompt dietary intake for immediate weight recovery, and provide an expedited chemotherapy and / or radiotherapy; which can be simply neoadjuvant or palliative, achieving a greater survival response [22]. It is important for the authors note that in our country there is no a mass method early diagnosis or screening for cancer of colon and rectum, although it is suspected that ranks the second place as a cause of death, which is alarming; therefore, the importance of the clinical history that in this manuscript is pointed and which allows only an indication of diagnosis in advanced stages, with a classical weight loss, rectal bleeding pain and altered bowel habits.
CONCLUSIONS
The LCA can occupy an innovative niche within the laparoscopic surgical approach, because the surgical technique here exposed and with the results obtained in the hospital, it proves to be quick, simple, effective, feasible, reproducible and safe, so it is unique. With a great evolutionary value in the surgical aspect and obviously in order to take care of our patients with a great clinical efficacy. Any sponsorship was received to carry out this study.
REFERENCES
- Harrell AG and Heniford BT. (2005). Minimally invasive abdominal surgery: lux et veritas past, present and future. Am J Sueg. 190(2), 239-243.
- McDermott JP and Corey TF. (1994). Laparoscopic appendicectomy- Review of the first decade. Irish Journal of Medical Science. 163(4), 171-172.
- Raynolds W Jr. (2001). The first laparoscopic cholecystectomy. JSLS. 5(1), 89-94.
- Jacobs M, Verdeja JC and Goldstein HS. (1991). Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc. 1(3), 144-150.
- Mukai M, Sadahiro S and Tokunaga N. (2007). Clinical experiences with laparoscopic colectomy. Digestive Endoscopy. 9(1), 11-15.
- Phillips EH, Franklin M and Carroll BJ. (1992). Laparoscopic colectomy. Ann Surg. 216(6), 703-707.
- Zucker KA. (2004). Laparscopic left hemicolectomy and sigmoidectomy. Laparoscopic surgery of the abdomen. 4, 369- 379.
- Benn PL, Wolff BG and Ilstrup DM. (1986). Level of anastomosis and recurrent colonic diverticulitis. Am J Surg. 151(2), 269-271.
- Boller AM and Nelson H. (2007). Colon and rectal cancer: Laparoscopic or open? Clinical Cancer Research. 13(22 pt 2), 6894.
- Inomata M, Yasuda K and Shiraishi N. (2009). Clinical evidences of laparoscopic versus open surgery for colorectal cancer. Clin Oncol. 39(8), 1063-1093.
- Gozález-Contreras QH and Rápalo H. (2008). Cirugía laparoscópica de colon y recto. Rev. Gastroenterol. Mex. 73(4), 203-208.
- Ramos JM, Beart Jr R and Goes R. (1995). Role of laparoscopy in colorectal surgery. A prospective evaluation of 200 cases. Diseases of the Colon and Rectum. 38(5), 494-501.
- Sireli P, Mele A and Stlfi VM. (2008). Incidence of adhesional small bowel obstruction after colorectal surgery. Asociación Americana Gastroenterológica. Digestive Disease Week.
- Kostener FL. (2004).Cirugía laparoscópica colorrectal: análisis de 85 pacientes consecutivos. Rev Chilena de Cirugía. 56:255-262.
- Senagore AJ, Dupree HJ and Delaney CP. (2003). Results of a standardized technique and postoperative care plan for laparoscopic sigmoid colectomy: a 30 -month experience. Dis Colon Rectum 46, 503-509.
- Tomita H, Marcello PW and Milson JW. (1999). Laparoscopic surgery of dhe colon and rectum.World Journal of Surgery. 23, 397-405.
- Dostalik J, Guková P and Martinrek L. (2006). Experiencia con colostomía laparoscópica. Cirujano General. 28(4), 234- 237.
- Nguyen HML, Causey MW and Steele SR. (2011). Single- Port laparoscopic diverting sigmoid colostomy. Diseases of dhe colon and rectum. 54(12), 1585-1588.
- Chen FM, Yin TC and Fan WC. (2012). Laparoscopic management for acute malignant colonic obctruction. Surgical laparoscopy endoscopy and percutaneous techniques. 22(3), 210-214.
- Tanaka E, Fukunaga Y and Nakashima M. (2015). Laparoscopic incisionless stoma creation for patients with colorrectalmalignant stricture. Surgical laparoscopy endoscopy and percutaneous techniques. 25(1), 37-39.
- 1. Blas FM, Delano AR and Pichardo FMA. (2010). Estomas por cirugía de mínima invasión, experiencia de cinco años, una alternativa quirúrgica segura. Cirugía Endoscópica. 11(3), 120- 128.
- Pittaluga M, Personnettaz E and Scala R. (2005). Colostomia laparoscópica:indicazioni e note di técnica chirurgica. G Chir. 26(3), 105-107.
- Hasegawa J, Hirota M and Kim HM. (2013). Single-incision laparoscopic stoma creation: Experience with 31 cases. Asian Journal of Endoscopic Surgery. 6(3), 181-185.
- 4. Rodriguez-Zentner H, Alemán-Loaiza E and Ríos JL. (2011). Hemicolectomía derecha laparoscópica por puerto único. Revista de Gastroenterología de México. 76(4), 364-365.
- Shah A, Moftah M and Nahar AF. (2014). Standardized technique for single port laparoscopic ileostomy and colostomy. Colorectal Disease. 16 (7), 248-252.
- Huynh H, Trottier DC and Soto CM. (2011). Laparoscopic colostomy reversal after a Hartmann procedure a prospective series, literatura review and an argument against laparotomy as the primary approach. Canadian Journal of Surgery. 54(2), 133-137.