Previous Issues Volume 2, Issue 2 - 2017
Joint Injuries Which Can Go Unnoticed: Fibular Head Dislocation
Abdullah Osman Kocak* , Ilker Akbas, Serdar Yasar
Department of Emergency Medicine, Faculty of Medicine, University of Ataturk, Erzurum, Turkey.
Corresponding Author: Abdullah Osman Kocak, Department of Emergency Medicine, Faculty of Medicine, University of Ataturk, 25240, Erzurum, TurkeyTel: +90 442 344 84 01; Fax: +90 442 236 31 33; E-Mail: [email protected]
Received Date: 30 Mar 2017 Accepted Date: 18 Apr 2017 Published Date: 21 Apr 2017
Copyright © 2017 Kocak OA
Citation: Kocak OA, Akbas I and Yasar S. (2017). Joint Injuries Which Can Go Unnoticed: Fibular Head Dislocation. Mathews J Emergency Med. 2(2): 024
INTRODUCTION Approximately 65% of the emergency cases are major and minor traumas. 35% of the unnoticed traumatic injuries are seen in the Emergency Departments. Unnoticed traumatic injuries adversely affects the patient's prognosis, as well as tarnishing the reliability and reputation of the related clinician and institution [1]. Dislocation of the Proximal Tibiofibular Joint (PTFJ) is among the injuries that can go unnoticed [2]. While dislocation of the PTFJ is usually described with accompanying bone fractures in the literature [3], isolated dislocation of the PTFJ is very rare [4]. This study aims to report an isolated PTFJ dislocation case presenting to our Emergency Department with the complaint of knee pain due to falling while walking.
CASE REPORT
A twenty eight year-old male patient presented to our Emergency Department with the complaint of knee pain due to a slip and fall accident on the accident. Physical examination revealed tenderness to palpation in the lateral aspect of the right knee. He was totally capable of passive movements of the joint; however, he felt increasing pain with the flexion of the knee and ankle. The patient could walk with support. His pulse palpations and neurological examination revealed normal results. Direct imaging suggested dislocation of the PTFJ (Figure 1). Then, computed tomography (CT) scan of the knee was performed.
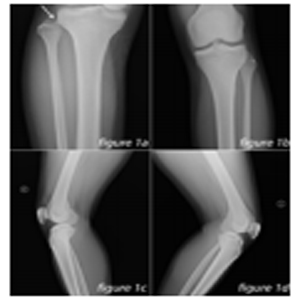
Figure 1: A. The anterior posterior radiograph of right lower extremity shows proximal tibiofibular joint dislocation (arrow); B. the anterior posterior radiograph of left lower extremity with normal findings; C. the lateral x-ray of right lower extremity demonstrate proximal tibiofibular joint dislocation; D. the lateral roentgenogram of left lower extremity with normal findings.
CT scan revealed anterolateral dislocation (Figure 2). Closed reduction was performed in the sedated patient using the conventional method with the collaboration of an orthopedic consultant in the Emergency Department, and long leg cast was applied. The patient was hospitalized in the Orthopedics Inpatient Clinic for monitoring and treatment. Magnetic resonance imaging (MRI) scan of the knee was performed to evaluate the ligament structures on Day 2 of hospitalization. Injury of the tibiofibular ligament was detected (Figure 3). Due to the absence of problems in his monitoring and follow-up results, the patient was discharged with recommendations on Day 5 of hospitalization.
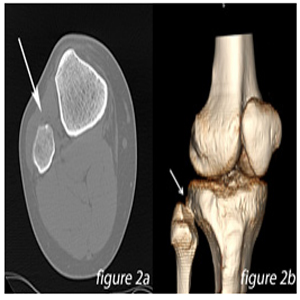
Figure 2: A. The axial section of right lower extremity computerized tomography demonstrate proximal tibiofibular joint dislocation and B. three-dimensional computerized tomography image shows proximal tibiofibular joint dislocation (arrows).
CT scan revealed anterolateral dislocation (Figure 2). Closed reduction was performed in the sedated patient using the conventional method with the collaboration of an orthopedic consultant in the Emergency Department, and long leg cast was applied. The patient was hospitalized in the Orthopedics Inpatient Clinic for monitoring and treatment. Magnetic resonance imaging (MRI) scan of the knee was performed to evaluate the ligament structures on Day 2 of hospitalization. Injury of the tibiofibular ligament was detected (Figure 3). Due to the absence of problems in his monitoring and follow-up results, the patient was discharged with recommendations on Day 5 of hospitalization.
DISCUSSION
Dislocation of the PTFJ was first described by Dubreuil in 1844. It is seen 3 times more commonly in men than in women (4). PTFJ varies anatomically depending on its angle relative to the horizontal plane. If the angle is < 200º, it is called the horizontal variant which is dislocation-resistant. If the angle is > 200°, it is called the oblique variant which constitutes 70% of the PTFJ dislocations [4, 5]. Consistent with the literature, our case had oblique type dislocation as well.
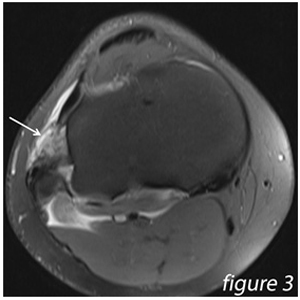
Figure 3: Magnetic resonance imaging of right lower extremity shows proximal tibiofibular joint dislocation (arrow).
The main stabilizer of PTFJ is tibiofibular ligament, the main component of the joint capsule. Since biceps femoris tendon and tibiofibular ligament reinforces the PTFJ capsule, this joint is very sound and strong [5]. Ogden described the dislocations under 4 types. Type I is the excessive anteroposterior movement without any true dislocation. Tip II is the anterolateral dislocation. This is the most common type accounting for 85% of all dislocation cases. Its mechanism consists of the external rotation of the leg, due to an abrupt internal rotation of the foot and plantar flexion, combined with knee flexion. Type III is the presence of posteromedial dislocation due to the direct blow to the head of the fibula. This type accounts for 10% of PTFJ dislocations. Type IV is usually the superior dislocation of the head of the fibula, accompanied by bone fracture, due to a high-energy trauma. Transient peroneal nerve injury may be seen in Types 2, 3 and 4 [6]. While our case had Type II dislocation, he did not have injury to the peroneal nerve. In the flexed position of the knee, fibular collateral ligament is relaxed and a rotary force applied at this moment strains the relaxed tibiofibular ligament which, in turn, results in an anterolateral dislocation [7]. MRI scan of our patient revealed injury to the tibiofibular ligament.
Dislocation of the PTFJ is a rare injury which can easily go unnoticed in direct imaging [2]. Diagnosis requires a high level of suspicion first. Usually, knee is capable of all kinds of movements which, however, can be restricted due to pain. Most patients have a hard time supporting their own body weight due to pain. Moving the ankle may increase the knee pain. While direct imaging scans are useful in first step investigations, they are not sensitive enough for diagnosis. Direct radiography findings in PTFJ dislocations are as follows: an increased laterodeviation of the head of the fibula and an enlarged interosseous region in AP aspect, and an increased anterior dislocation of the head of the fibula in lateral radiography [5].
In addition to the direct imaging scans, axial CT scan may be useful in that it helps verify the dislocation, determine the direction of dislocation, find out about the condition of the joint, and detect additional pathologies. Diagnostic sensitivity of axial CT is %86. MRI scan may help diagnose the atypical cases, and it helps show the ligament integrity and fluid collections [4].
All 4 types of dislocations can be treated with closed reduction procedure. While this procedure may be performed in Emergency Departments by administering local anesthesia or sedoanalgesics, it may also be performed in operating rooms using general anesthesia [5]. Anterolateral, posterior and superior dislocations for which closed reduction procedures have failed are detected surgically [2]. If the dislocation is identified, it can easily be treated in the Emergency Department without any surgery [2]. The most common closed reduction method was described by Ogden. First, the physician renders the foot dorsiflexed and rotates it externally and tries to rotate the fibula externally. Then, the knee is flexed up to 70-110 degree and reduction is performed by applying pressure on the head of the fibula at the same time [8]. Based on the physical examination and direct imaging results of our case, we performed CT scan due to the suspicion of PTFJ dislocation. Upon the final diagnosis with CT scan, an MRI scan was performed to evaluate the condition of the ligament structures. MRI scan revealed injury to the tibiofibular ligament. Furthermore, our case had early intervention with early diagnosis and he was treated and discharged without surgery.
CONCLUSION
PTFJ dislocations should be considered in the distinctive diagnosis of the patients with posttraumatic knee pain. Early diagnosis and urgent reduction of the acute dislocation of the proximal tibiofibular joint is important for preventing longterm complications. If this rarely seen clinical case which can be easily reduced in the Emergency Department goes unnoticed, it will lead to extra surgical intervention, morbidity and unnecessary treatment costs.
REFERENCES
- Emet M, Saritas A, Acemoglu H, Aslan S, et al. (2010). Predictors of missed injuries in hospitalized trauma patients in the emergency department. European journal of trauma and emergency surgery: official publication of the European Trauma Society. 36(6): 559-566.
- Horan J and Quin G. (2006). Proximal tibiofibular dislocation. Emergency medicine journal: EMJ. 23(5): e33.
- Calabro T, Cevolani L, Chehrassan M and Gasbarrini A. (2014). A new technique of reduction for isolated proximal tibiofibular joint dislocation: a case report. Eur Rev Med Pharmacol Sci. 18(1Suppl): 93-95.
- Klaunick G. (2010). Recurrent idiopathic anterolateral dislocation of the proximal tibiofibular joint: case report and literature review. Journal of pediatric orthopedics Part B.19(5): 409-414.
- Van Seymortier P, Ryckaert A, Verdonk P, Almqvist KF, et al. (2008). Traumatic proximal tibiofibular dislocation. The American journal of sports medicine. 36(4): 793-798.
- Ogden JA. (1974). Subluxation and dislocation of the proximal tibiofibular joint. The Journal of bone and joint surgery American volume. 56(1): 145-154.
- Robinson Y, Reinke M, Heyde CE, Ertel W, et al. (2007). Traumatic proximal tibiofibular joint dislocation treated by open reduction and temporary fixation: a case report. Knee Surg Sports Traumatol Arthrosc. 15(2): 199-201.
- Ogden JA. (1974). Subluxation of the proximal tibiofibular joint. Clinical orthopaedics and related research. (101): 192-197.