Previous Issues Volume 1, Issue 1 - 2016
Intestinal Intussusception by Syndrome Attenuated Familial Adenomatous Polyposis
Morelos Adolfo Garcia Sánchez1, Mireya De La Fuente González1, Fausto Romero Vallejo1, Álvaro Tomás Ruz Concha1, José Martin Díaz Ramírez1 , Irving Dolores García1, Erika Berenice Ramírez Pérez1, Gustavo Armando Santillán Cisneros1, Laura Guadalupe Valdez Sánchez1
Corresponding Author: Morelos Adolfo Garcia Sánchez,1Gaudencio Gonzalez Garza General Hospital Specialized Medical Unit, at La Raza National Medical Center, IMSS.-Mexican Social Security Institute. address Avenida de las Jacarandas y Calzada Vallejo s/n. Colonia La Raza, Delegacion Azcapotzalco, C.P. 02990. México, Tel: 01 (52) 5524-5900; Email:[email protected]
Received Date: 13 Oct 2016 Accepted Date: 12 Dec 2016 Published Date: 15 Dec 2016
Copyright ©2016 Garcia MA
Citation: García SMA,De La Fuente GM, Romero VF, Ruz CAT, et al. (2016). Intestinal Intussusception by Syndrome Attenuated Familial Adenomatous Polyposis.Mathews J Gastroenterol Hepatol 1(1): 006.
ABSTRACT
Intestinal intussusception (ININ) in adults is very rare, and associated to Attenuated familial adenomatous polyposis (AFAP) is even more. A clinical case is presented which perhaps is the first case reported so far. Its diagnostic complexity and its prevention null is mentioned too, by a certain community galenica AFAP ignorance. And his poor prognosis is for a very late diagnosis. Although this treatment is surgical, the role of endoscopic services and expertise to be operation is essential. The other factor that it comes with, is the hospital infrastructure that directly affects the notarization, resolution and prognosis. Hence the importance of publicizing our experience.
INTRODUCTION
The intestinal intussusception (ININ) in adult people is very rare and its etiology, is multiple as diverse, which consists of introducing a intestine segment within another through peristalsis in an extensive worldwide literature review so far the authors have not found an etiological description of ININ due to Attenuated familial adenomatous polyposis (FAPA); perhaps because they are rare, being a “recently described” and even unknown pathology [1, 2]. AFAP was recognized in 1995 by Henry Lynch and is characterized [3-5].
- Mild-variant of familial adenomatous polyposis (FAP).
- Less Than 100 polyps, average 50.
- No Phenotypic expression.
- Antecedent family.
- Polipos In extracolonic intestinal tract.
AFAP is an inherited autosomal dominant disease by germline mutations in the 5’and 3’ ends of the APC gene [2, 4, 5]. Its incidence is unknown; the clinical symptoms are not typical and it depends on the number of polyps, the diagnoses usually is because of discovering or due to another medical reason, related to the age, personal and family history [2, 3].
CASE REPORT
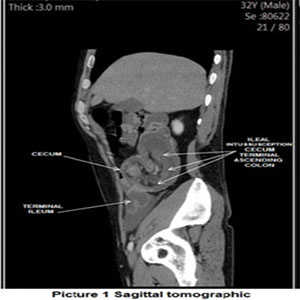
We report the case of a 32 years old male patient with a father's dead background because of “tumor” in colon at the age of 41 years old. The Patient presents 4 days of developing of a severe abdominal pain, cramping, nausea, vomiting, abdominal distension, diarrhoea, intermittent fever, with clinical symptoms of acute abdomen, which corresponds to general abdominal pain, incapacitant, with nausea, vomiting, absence of gas canalization, fever, attacking the general state with asthenia and adinamia, with systemic inflammatory response data, to physical exploration with a sign of peritoneal irritation and pain intensive wing palpation. which urges surgical treatment a computed tomography is performed (ct), where an invagination of ileum was observed in the cecum Figure 1.
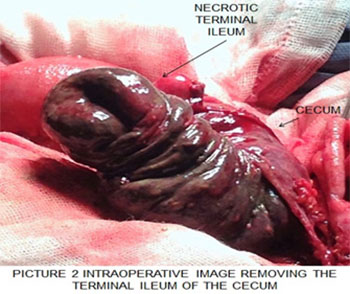
It undergoes a emergency surgery finding a generalized peritonitis, with “a mass or block of inflammatory nature” of 15x20x12 cm in diameter per ININ of cecum ileum of 15 cm in lenght with ileal necrosis and up to 10 cm cecum ascending colon Figure 2.
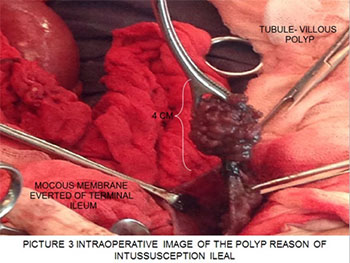
In the intraoperatively 3 villous polyps are located at 5 cm in the remaining ileum, which are resected Figure 3.
It is performed a right hemicolectomy with resection of 25 cm of terminal ileum and ileostomy. The postoperative was torpid with intestinal malabsorption syndrome, emerging the ileostomy, giving a medical treatment to the patient with an appropriate response, which consists in total parenteral nutrition as well as elemental diet (mixed nutrition) which progressed to a semielemental diet, a polymeric and a normal diet. it is appliced therapy with loperamide maximum doses 20 mgs a day, butilhioscina doses of 30 mgs a day distributed in three doses, pulses of methylprednisolone 100 mgs each 8 hrs for 10 days, octeotride subcutaneous 10 micrograms c / 8 hrs, all this in a month. It is protocolised performing panendoscopy with a report of 2 duodenal polyps and a periampullary of 1 to 2 cm adenomatous aspect; enteroscopy detects two pedicle jejunal polyps 2 cm tubule-villous aspect which are resected, and colonoscopy with a polyp more in the remainder of the transverse colon if 1 cm which has a villous appearance, then is performed a polypectomy.
The pathology report describes
“villous tubule-ileocecal valve with tubulo-villous adenoma with high-grade dysplasia, a segment of colon and terminal ileum with necrosis and transmural ischemic damage. Duodenal polyps tubule-villous with high-grade displasia. Jejunal polyps with dysplasia high grade. And colonic polyp with carcinoma in-situ. “The genetic study confirmed the diagnosis of AFAP. The following are: code 16930 loss or duplication of the APC1 gene, code 16934 gene sequence APC1, code91461 Lynch 1 Syndrome Panel which includes mutational tests of MLH1, MSH2, MSH6, PMS2, and loss of 3’-EPCAM.It is derived from the oncology department for handling.
DISCUSSION
In this study two extremely rare pathologies are described. AFAP is a relatively “new” disease in its description, so it is difficult associated it with ININ as their cause. The ININ is very rare, represents a 1 to 5% of intestinal obstructions, it is more associated with malignancy in their etiology in colon, idiopathic in 10% and small intestine the most are benign by 60% [6-8]. The clinical symptoms may present a chronic non-specific or intermittent abdominal pain, but also acutely and in others, with typical data bowel obstruction; confirmed or detected by CT, or failing in the same surgery [7- 9]. Clinical is such as unspecific. Which leads to a very difficult diagnosis and torpid [8]. The treatment is surgery or conventional laparoscopic surgery, with en bloc resection in almost all cases [7, 9, 10, 11].
The authors conclude
The ININ is a “game of pressure”; only exist peristalsis but that is not sufficient, but also the presence of an increased surface (the tumor), and decreased diameter of intestinal gauge which increases the pressure, with a force of persistent and continues pressure (peristalsis) which causes the ININ in adults. The so-called tumor that in a large percentage is malignant occurs acutely in the ININ, this is obvious and its growth is exponential, fast and well vascularized. Regarding the AFAP its diagnosis is difficult and even more if it is not suspicion or not well known, with a high malignancy potential and a poor prognosis. Treatment is diverse and it just focus on the consequences or isolated findings at the time of diagnosis: colectomy, pancreaticoduodenectomy, endoscopic follow-up and multiple polypectomies [2]. Although exist studies approved as adjunctive therapy with celecoxib so far, which reduces the risk of developing cancer of adenomatous polyps [12]. And its previous diagnosis delay, in asymptomatic patients is currently up to 15 years drastically poorer prognosis; it is also important to note that colonoscopy takes precedence over sigmoidoscopy and monitoring must be for life, in most patients,“prophylactic” colectomy and ileo-rectal anastomosis. It is recommended at the age of 20 to 25 years [13, 14]. It is important to note that there are many limitations in our medical environment, especially hospital infrastructure, the low index of clinical suspicion and the difficulty in identifying a specific genetic mutations lead to a late, incomplete and poor prognosis diagnosis and therefore a treatment that in the most of time it is only palliative. It is essential the disclosure of clinical cases like this that make us know the characteristics of both pathologies, trying to make a complete diagnostic approach, and to anticipate possible complications with genetic counseling to the family. So make the change, to improve the prognosis and quality of life, the future of our patients.
REFERENCES
- Franco-Herrera R, Burneo-Esteves M, Martin- Gil J, Fabregues- Olea A, et al. (2012). Intussusception in adults. A rare cause of mechanical obstruction. Journal of Gastroenterology of Mexico. 77(3), 153-156.
- Tieu H, Edelstein D, Axilbund J, Romans KE, et al. (2015). Clinical Characteristics of Multiple Colorectal Adenoma Patients Without Germline APC or MYH Mutations. Journal of Clinical Gastroenterology. 50(7), 584-588.
- . Castro JM, Martínez EC, Hormaza JA, Lina M, et al. (2004). Attenuated familial adenomatous polyposis. Controversial entity. 19(3), 123-127.
- Fernandes GO, Pereira JJ and Franca MAV et al. (2007). Attenuated familial adenomatous polyposis. Rev. Bras. Colo- Proctol. 27, 179-184.
- Marafie MJ, Al-Elwani Fl and Al-Suliman IS. (2014). Familial adenomatous polyposis: two different APC gene mutations in two unrelated Arab families with differing response to genetic counselling. Middle East Journal of Medical Genetics. 3, 31-36.
- 6. Koskenvuo L, Peltomáki P, Renkonen-Sinisalo L, Gylling A, et al. (2016). Desmoid Tumor Patients Carry an Elevated Risk of Familial Adenomatous Polyposis. Journal of Surgical Oncology. 113(2), 209-212.
- Siow SL and Mahendran HA. (2014). A Case Series of Adult Intussusception Managed Laparoscopically. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques. 24(4), 327-331.
- Cristóbal-Poch L, Trébol-López J and Gónzalez-Gómez C.(2015). Colic intussusception in adults. Our experience in 13 years. Rev Acircal. 2, 28-46.
- Ma KW, Li WH and Cheung MT. (2012). Adult intussusception: A 15-year retrospective review. Surgical Practice. 16(1), 6-11.
- Van DL, Noordman BJ, Scheepers JJ and Hartholt KA. (2015). A young woman with a jejuno-jejunal intussusception. BMJ Case Reports.
- Emet M, Kocak AO, Akbas I, Arslan S, et al. (2015). Spontaneous reduction of ileoileal adult intussusception after blunt abdominal injury. American Journal of Emergency Medicine. 33, 1542e3-1542e5.
- Hanan B, Diniz T R, Da L, Da CSA, et al. (2010). Intussusception in adults: a retrospective study. Colorectal Disease. 12(6), 574-578.
- Lynch PM, Burke CA, Phillips R, Morris, et al. (2016). An international randomised trial of celecoxib versus celecoxib plus difluoromethylornithine in patients with familial adenomatous polyposis. Gut. 65(2), 286-295.
- . Knudsen AL, Bülow S, Tomilson I, Möslein G,et al. (2010). Attenuated familial adenomatous polyposis: results from an international collaborative study. Colorectal Dis. 12, 243-249.