Previous Issues Volume 3, Issue 1 - 2018
Impact of Etonogestrel Subdermal Implant Versus Depot-Medroxyprogesterone Acetate Injection on Menstrual Changes And Uterine Artery Doppler Indices: A Randomized Clinical Trial
Mohamed Rezk¹*, Osama Elkelani¹, Haitham Hamza¹, Mohamed Shawky2 , Hala Marawan³
1Department of Obstetrics and Gynecology, Egypt 2Department of Radiology, Egypt. 3Department of Public Health and Community Medicine, Faculty of Medicine, Menoufia University, Egypt. Corresponding Author: Mohamed Rezk, 25 Yasin Abdelghafar street, Shibin ElKom City, Menoufia governorate, Egypt, Tel:+201146256413; Email: [email protected]
Received Date: 05 Jan 2018 Accepted Date: 21 Feb 2018 Published Date: 23 Feb 2018
Copyright © 2018 Rezk M
Citation: Rezk M, Elkelani O, Hamza H, Shawky M, et al. (2018). Impact of Etonogestrel Subdermal Implant Versus Depot-Medroxyprogesterone Acetate Injection on Menstrual Changes And Uterine Artery Doppler Indices: A Randomized Clinical Trial. Mathews J Gynecol Obstet. 3(1): 14.
ABSTRACT
Objective: To ascertain the impact of Etonogestrel subdermal implant (ENG-implant) versus Depot-medroxyprogesterone acetate injection (DMPA) on menstrual changes and uterine artery Doppler indices at 3 and 6 months after use and to assess the association between menstrual irregularities among the new users and Doppler changes in uterine arteries. Methods: 311 multiparous women were randomly allocated into two types of progestin-only contraception, group 1 received the ENG implant (n=152) and group 2 received DMPA (n=159). Women were followed for 6 months with assessment of uterine artery pulsatility index (PI) and resistant index (RI) initially then at 3 and 6 months after insertion. Multiple logistic regression analysis of participants’ characteristics and Doppler indices was done for correlation with menstrual changes.
Results: Abnormal bleeding affected 27.6% in the ENG implant group and 34.6% in the DMPA group while amenorrhea affected 21.1% in the ENG implant group compared to 30.2% in the DMPA group (p>0.05). Uterine artery PI was significantly correlated with abnormal bleeding at cut off value of 1.35 with AUC 0.93, sensitivity 88% and specificity 100% while RI at cut off value of 0.62 with AUC 0.1, sensitivity 96% and specificity 100%. Uterine artery PI was significantly correlated with amenorrhea at cut off value of 2.25 with AUC 100, sensitivity 100% and specificity 96% while RI at cut off value of 0.82 with AUC 98, sensitivity 100% and specificity 85%.
Conclusion: Menstrual changes among new users of ENG implant and DMPA is associated with changes in the uterine artery blood flow.
KEYWORDS
Menstrual Changes; Etonogestrel Subdermal Implant; Depot-Medroxyprogesterone Acetate; Abnormal Bleeding; Amenorrhea.
INTRODUCTION
Progestin-only contraceptives are longer-acting highly effective methods that can be used by most women in most situations. About 6% of women use injectables while 1% use implants all over the world [1-4].Provision of both Injectables and implants to women can be achieved at any time during the menstrual cycle after exclusion of pregnancy, which can be ruled out by a pregnancy test [1].
Menstrual changes in the form of amenorrhea or various bleeding patterns (vaginal spotting, heavy bleeding, irregular or prolonged bleeding) are the main causes of discontinuation of hormonal contraceptive methods [5].
Progestin only methods are associated with more menstrual irregularity than the combined methods. Most women using progestin-only methods will suffer irregular bleeding patterns during the first year of use, although such irregularity will be reduced over time [6, 7].
The use of DMPA is associated with amenorrhea which rises over time from 40-50% after 1 year to about 80% after 5 years of continuous use while the use of ENG implants is associated with fewer bleeding episodes and significantly higher rates of amenorrhea [8, 9]. To the authors’ knowledge, no prior studies in the literature explored the impact of ENG implant on uterine blood flow.
The aim of this study was to ascertain the impact of Etonogestrel subdermal implant (ENG-implant) versus Depot-medroxyprogesterone acetate injection (DMPA) on menstrual changes and uterine artery Doppler indices at 3 and 6 months after use and to assess the association between menstrual irregularities among the new users and Doppler changes in uterine arteries.
MATERIALS AND METHODS
This randomized parallel group study was carried out at the Department of Obstetrics and Gynecology in collaboration with the Radiology and Public Health and Community Medicine departments, during the period between the middle of December 2016 and the end of August 2017.
Ethical approval of the study protocol was obtained (Ethical clearance letter number 459M/2016) in accordance with the 1964 Helsinki declaration and its later amendments. All participants signed the informed consent form prior to commencing the study.
Following complete history taking, clinical examination and transvaginal ultrasonography, multiparous women with normal menstrual cycle who requested long acting reversible contraception (LARC) and fulfilled the criteria for progestin administration were enrolled. Both ENG implant and DMPAIM are freely available at our family planning clinic.
Nulliparity, pregnancy, undiagnosed uterine bleeding, past or current history of breast cancer, liver disease, medical disorders and any contraindication to progestin administration were listed as exclusion criteria. Nullipara in Egypt decline to use any method of contraception because of fear about future fertility. groups regarding the occurrence of irregular uterine bleeding during the first 6 months after use, One hundred and fifty patients were required in each group for the study to have 80% power at the 5% significance level. We primarily included 165 participants in each group with extra 10% for possible drop out cases. At the 6th month visit, 311 multiparous women completed the study
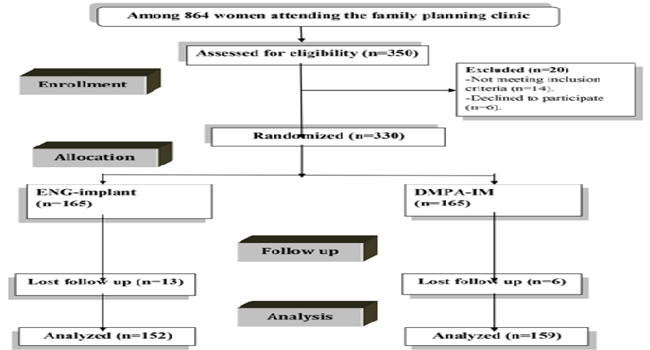
Figure 1: CONSORT Flow Diagram.
Randomization in 1:1 ratio was carried out using computergenerated simple random tables with women allocated into one of the two groups:
Group 1(Etonogestrel subdermal implant, ENG- group) comprised 152 women to whom ENG implant (Implanon 68 mg, N.V. Organon, Oss, The Netherlands) was inserted.
Group 2 (Depot-medroxyprogesterone acetate, DMPAgroup) comprised 159 women who used DMPA 150mg (Depo Provera, Pfizer, USA) by IMI every 3 months. Uterine artery Doppler study was performed at the Radiology department before starting the method and at 3 months and 6 months thereafter, using a Hitachi EUB-7000 ultrasound machine (Hitachi, Japan) by 7 MHz transvaginal probe. Examinations were done by a single operator with previous experience in Doppler ultrasound to avoid inter-observer variability who was blinded to the used method for contraception. Pulsed wave Doppler was applied at a sampling gate of 2 mm with the angle of insonation at less than 30°. Pulsatility index (PI) and Resistance index (RI) were determined automatically following three similar waveforms in both uterine arteries with recording of the average readings. Women were instructed to avoid the intake of non-steroidal anti-inflammatory drugs 24 hours before the examination. All the ultrasound Doppler studies were measured between 8:00 and 11:00 am to eliminate diurnal variation.
At 4 weeks from the procedure, the patient was asymptomatic and reported a straight and continuous urinary stream. Patient had not yet engaged in sexual intercourse. The cystic walls remained collapsed (Figure 2). Histology revealed benign findings (Figure 3).
OUTCOME MEASURES
Primary outcome
Menstrual changes and changes in uterine artery Doppler indices after 3 and 6 months of use. - Correlation between uterine artery Doppler and subsequent irregular bleeding or amenorrhea.
Secondary outcome
Adverse effects of the method, continuation rate at 6 months and patient acceptability. Menstrual calendars were used to record the days on which women suffered bleeding as recommended by the World Health Organization (WHO). A bleeding episode is defined as the period of consecutive bleeding days, while a bleeding-free interval is the period of consecutive bleeding-free days and a menstrual segment is defined as a bleeding episode and the subsequent bleeding-free interval. Spotting was defined as very slight bleeding that required no sanitary protection, whereas heavy bleeding did require sanitary protection. Women acceptability in terms of compliance with follow-up, overall satisfaction and recommendation of the method to other women, was assessed at 6 month follow up visit via predesigned questionnaire.
Inquiry about adverse effects was done at each scheduled visit with an appropriate undertaking management of symptoms. Women were also instructed to attend the hospital to rule out pregnancy in the event of a missed period, severe lower abdominal pain (to exclude ectopic pregnancy), heavy vaginal bleeding, or signs of infection at the ENG implant insertion site.
STATISTICAL ANALYSIS
The data were tabulated, and analyzed by SPSS (statistical package for social science) version 22 on IBM compatible computer (SPSS Inc., Chicago, IL, USA).
Two types of statistics were done • Descriptive statistics (Number, percentage (%), median and interquartile range) • Analytic statistics: which include the following tests: Chisquare test (x2): was used to study association between two qualitative variables. Mann-Whitney- test for comparison between two independent quantitative variables. P-value of <0.05 was considered statistically significant. Multiple logistic regression was done to determine predictors of abnormal bleeding or amenorrhea. Receiver operator characteristic (ROC) curve was done to determine Cut –off value, sensitivity and specificity of PI and RI in diagnosis of bleeding or amenorrhea.
RESULTS
There was no significant difference between the two groups regarding age, parity and body mass index as depicted in table (1).
Table 1: Participants' characteristics
| ENG implant group(n=152) | DMPA group(n=159) | Student t-test | P-value | |
|---|---|---|---|---|
| Age (year) | 32.1±3.39 | 31. 9±3.49 | 0.51 | >0.05 |
| Parity | 2.78±1.01 | 2.69±1.16 | 0.738 | >0.05 |
| Body mass index (Kg/m²) | 24.9±2.98 | 25.1±3.18 | 0.57 | >0.05 |
Uterine artery PI and RI were shown in table (2).
Table 2: Uterine artery Pulsatility Index (PI) and Resistance Index (RI).
| ENG implant group(n=152) | DMPA group (n=159) | Mann-Whitney test | P-value | |
|---|---|---|---|---|
| Initial PI PI after 3 months P value from initial PI after 6 months P value from initial | 2.1(1.9-2.3) | 1.9(1.2-3.6) | 1.74 | >0.05 |
| 1.9(1.3-2.2) <0.001 | 1.9(1.2-3.7) <0.001 | 1.09 | >0.05 | |
| 1.9(1.4-2.17)<0.001 | 1.9(1.2-3.8) <0.001 | 0.850 | >0.05 | |
| Initial RI RI after 3 months P value from initial RI after 6 months P value from initial | 0.77(0.71-0.82) | 0.76(0.62-0.84) | 2.35 | >0.05 |
| 0.77(0.62- 0.80) <0.001 | 0.80(0.61- 0.88) (<0.001) | 0.155 | >0.05 | |
| 0.76(0.63- 0.83) <0.001 | 0.80(0.60- 0.89) <0.001 | 0.354 | >0.05 |
There was no significant difference between the two groups regarding uterine artery PI and RI initially, at 3 months and at 6 months (p>0.05). There was a highly significant difference in every single group regarding PI and RI at 3 and 6 months when compared to the initial Doppler indices (p<0.001).
Table 3: Multiple logistic regression analysis of participants' characteristics and menstrual changes.
| Chi square of regression | P-value | Odd's ratio | 95%CI | |
|---|---|---|---|---|
| Abnormal bleeding: | ||||
| Age | 0.012 | 0.912 | 0.944 | 0.892-1.11 |
| BMI | 0.119 | 0.730 | 0.985 | 0.904-1.07 |
| Uterine PI | 13.21 | <0.001 | 5.86 | 2.25-15.2 |
| Uterine PI | 21.47 | <0.001 | 8.25 | 2.79-17.63 |
| Parity | 0.242 | 0.623 | 0.930 | 0.69-1.24 |
| Amenorrhea: | ||||
| Age | 0.002 | 0.96 | 1.003 | 0.89-1.12 |
| BMI | 0.024 | 0.87 | 0.993 | 0.904-1.08 |
| Doe | 80 | Doe | 80 | 80 |
| Uterine PI | 7.92 | <0.001 | 2.133 | 1.75-4.39 |
| Uterine RI | 5.44 | <0.05 | 1.99 | 0.93-2.17 |
| Parity | 0.68 | 0.79 | 0.95 | 0.701-1.31 |
Uterine artery PI was significantly correlated with abnormal bleeding at cut off value of 1.35 with area under the curve (AUC) of 0.93 with sensitivity of 88% and specificity of 100% while uterine artery RI was significantly correlated with abnormal bleeding at cut off value of 0.62 with AUC of 0.1 with sensitivity of 96% and specificity of 100%.
Uterine artery PI was significantly correlated with amenorrhea at cut off value of 2.25 with AUC of 100 with sensitivity of 100% and specificity of 96% while uterine artery RI was significantly correlated with amenorrhea at cut off value of 0.82 with AUC of 0.1 with sensitivity of 100% and specificity of 85% as revealed in table (4).
Table 4: Multiple logistic regression analysis of participants' characteristics and menstrual changes.
| Uterine artery PI | I Uterine artery RI | |
|---|---|---|
| Abnormal bleeding: | ||
| AUC | 0.93 | 100 |
| Cut –off value | 1.35 | 0.62 |
| Sensitivity | 88 | 96 |
| Sensitivity | 100 | 100 |
| Amenorrhea: | ||
| AUC | 100 | 0.98 |
| Cut –off value | 2.15 | 0.82 |
| Sensitivity | 100 | 100 |
| Sensitivity | 96 | 85 |
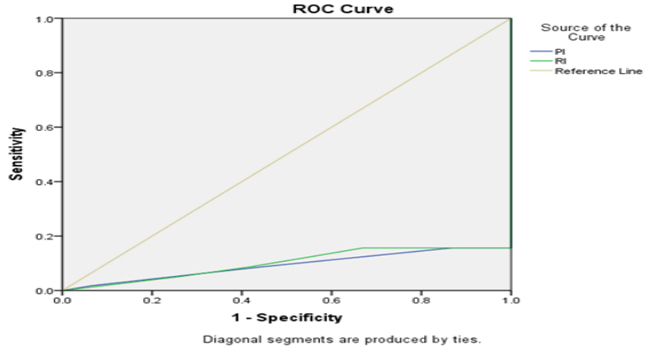
Figure 2: ROC curve between uterine artery PI and RI and abnormal bleeding.
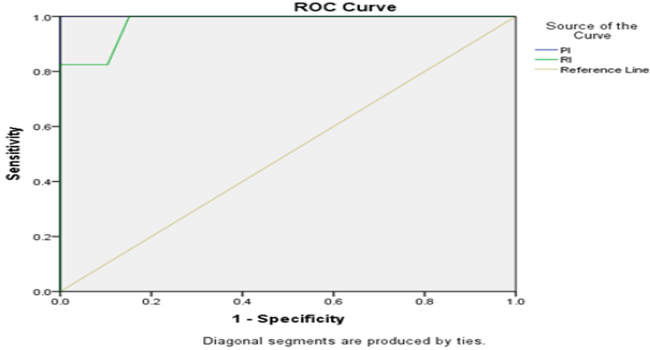
Figure 3: ROC curve between uterine artery PI and RI and amenorrhea.
Abnormal bleeding affected 27.6% in the ENG implant group compared to 34.6% in the DMPA group (p>0.05) while amenorrhea affected 21.1% in the ENG implant group compared to 30.2% in the DMPA group (p>0.05). Continuation rate at 6 months was 88.2% in the ENG implant group compared to 89.3% in the DMPA group (p>0.05). Women in both groups expressed high acceptability for the used contraceptive method (p>0.05).
DISCUSSION
Abnormal bleeding affected 27.6% in the ENG implant group compared to 34.6% in the DMPA while amenorrhea affected 21.1% in the ENG implant group compared to 30.2% in the DMPA group. Uterine artery PI and RI were significantly correlated with menstrual changes in both groups at 3 and 6 months. Continuation rate at 6 months was 88.2% in the ENG implant Table (5) depicts adverse effects, continuation rate and women acceptability.
Table 5: Adverse effects, continuation rate and acceptability.
| ENG implant group (n=152) | DMPA group (n=159) | Chi square test | P-value | |
|---|---|---|---|---|
| Menstrual changes: | ||||
| -Abnormal bleeding | 42(27.6%) | 55(34.6%) | 1.75 | >0.05 |
| At 3 months | 30 | 40 | ||
| At 6 months | 12 | 15 | ||
| -Amenorrhea | 32(21.1) | 48(30.2%) | 3.39 | >0.05 |
| At 3 months | 15 | 18 | ||
| At 6 months | 18 | 30 | ||
| Abdominal pain | 14(9.2%) | 18(11.3%) | 0.18 | >0.05 |
| Weight changes | 22 (14.5%) | 28(17.6%) | 0.36 | >0.05 |
| Headache | 16(10.5%) | 12(7.5%) | 0.52 | >0.05 |
| Asthenia (weakness or fatigue) | 14(9.2%) | 12(7.5%) | 0.11 | >0.05 |
| Decreased libido | 8(5.3%) | 12(7.5%) | 0.35 | >0.05 |
| Pelvic pain | 10(6.6%) | 10(6.3%) | 0.02 | >0.05 |
| Breast pain | 40(26.3%) | 25(15.7%) | 5.27 | >0.05 |
| Continuation rate at 6 months | 134(88.2%) | 142(89.3%) | 0.02 | >0.05 |
| >0.05 | 136(89.5%) | 144(90.6%) | 0.02 | >0.05 |
| Recommendation to others | 132(86.8%) | 142(89.3%) | 0.25 | >0.05 |
| Overall satisfaction | 134(88.2%) | 142(89.3%) | 0.02 | >0.05 |
group compared to 89.3% in the DMPA group. Women in both groups expressed high acceptability for the used contraceptive method. No prior studies addressed the changes in uterine artery PI and RI among ENG implant users with previous three studies [10-12] reported changes among DMPA users. A previous observational study conducted on 50 women, 25 using LNG-IUS and 25 using DMPA, has revealed lower subendometrial vascularisation and higher PI in the spiral arteries among DMPA-users [10]. Another smaller study conducted on 40 women using DMPA; 20 with amenorrhea and 20 with abnormal bleeding, revealed a significant reduction of uterine artery PI and RI in the uterine artery among users suffered irregular uterine bleeding [11].
Our recent observational study [12] have demonstrated a positive linkage between DMPA use (n=104) and changes in uterine artery PI and RI indices, which were reduced in users who suffered from abnormal bleeding and elevated in users who experienced amenorrhea. Implanon use was associated variable menstrual changes as amenorrhea (22.2%) and infrequent (33.6%), frequent (6.7%), and/or prolonged bleeding (17.7%) as reported in a previous review of data from 11 clinical trials [6]. Previous studies have demonstrated a high continuation rate for ENG implant at 6 and 12 months of about 90% among new users [13-15]. Also, the overall satisfaction for both ENG implant and DMPA was reported by earlier studies [16,17]. The study design and the larger number of participants constitute the main strength of the current study. Inability to extend the period of follow up was unintended limitation of this study. Future research should focus on the predictive value of uterine artery Doppler indices and subsequent menstrual changes among new users. Uterine artery Doppler study is simple, inexpensive and readily available tool to assess women with menstrual changes following the use of ENG implant or DMPA for contraception. Effective counseling on the possible menstrual changes among new users is mandatory to improve continuation rates.
CONCLUSION
Menstrual changes among new users of ENG implant and DMPA is associated with changes in the uterine artery blood flow.
CONFLICT OF INTEREST
Non-Declared.
REFERENCES
- (2004). World Health Organization. Selected practice recommendations for contraceptive use. 2nd ed. Geneva: World Health Organization.
- Darney P, Patel A, Rosen K, Shapiro LS, et al. Safety and efficacy of a single-rod etonogestrel implant (Implanon): results from 11 international clinical trials. Fertil Steril. 91(5): 1646-1653.
- Kaunitz AM, Darney PD, Ross D, Wolter KD, et al. (2009). Subcutaneous DMPA vs. intramuscular DMPA: a 2-year randomized study of contraceptive efficacy and bone mineral density. Contraception. 80(1): 7-17.
- Winner B, Peipert JF, Zhao Q, Buckel C, et al. (2012). Effectiveness of long-acting reversible contraception. N Engl J Med. 366(21): 1998-2007.
- Grunloh DS, Casner T, Secura GM, Peipert JF, et al. (2013). Characteristics associated with discontinuation of longacting reversible contraception within the first 6 months of use. Obstet Gynecol. 122(6): 1214-1221.
- Mansour D, Korver T, Marintcheva-Petrova M and Fraser IS. (2008). The effects of Implanon on menstrual bleeding patterns. Eur J Contracept Reprod Health Care. 13(Suppl. 1): 13-28.
- Bachmann G and Korner P. (2009). Bleeding patterns associated with non-oral hormonal contraceptives: a review of the literature.Contraception. 79: 247e58.
- Darney P, Patel A, Rosen K, Shapiro LS, et al. (2009). Safety and efficacy of a single-rod etonogestrel implant (Implanon): results from 11 international clinical trials. Fertil Steril. 91(5): 1646-1653.
- Hubacher D, Lopez L, Steiner MJ and Dorflinger L. (2009). Menstrual pattern changes from levonorgestrel subdermal implants and DMPA: systematic review and evidencebased comparisons. Contraception. 80(2): 113-118.
- Dane B, Akca A, Dane C, Evcimen S, et al. (2009). Comparison of the effects of the levonorgestrel-releasing intrauterine system (Mirena) and depot-medroxyprogesterone acetate (Depo-Provera) on subendometrial microvascularisation and uterine artery blood flow. Eur J Contracept Reprod Health Care. 14(3): 240-244.
- Hussein M. (2011). Transvaginal Doppler sonography for evaluation of irregular uterine bleeding with DMPA. Arch Gynecol Obstet. 283(6): 1325-1328.
- Rezk M, Al-Halaby A, Emarh M and Shawky M. (2017). Correlation between uterine artery Doppler indices and menstrual irregularities among levonorgestrel releasing intrauterine system and depot medroxyprogesterone acetate users: a prospective observational study. Eur J Contracept Reprod Health Care. 22(4): 316-320.
- Lakha F and Glasier AF. (2006). Continuation rates of Implanon in the UK: data from an observational study in a clinical setting. Contraception. 74(4): 287-289.
- Bhatia P, Nangia S, Aggarwal S and Tewari C. (2011). Implanon: subdermal single rod contraceptive implant. J Obstet Gynaecol India. 61(4): 422-425.
- Berenson AB, Tan A and Hirth JM. (2015). Complications and continuation rates associated with 2 types of longacting contraception. Am J Obstet Gynecol. 212(6): 761. e1-8.
- Short M, Dallay D, Omokanye S, Hanisch JU, et al. (2012 ). Acceptability of the levonorgestrel releasing-intrauterine system and etonogestrel implant: one-year results of an observational study. Eur J Contracept Reprod Health Care. 17(1): 79-88.
- Diedrich JT, Desai S, Zhao Q, Secura G, et al. (2015). Association of short-term bleeding and cramping patterns with long-acting reversible contraceptive method satisfaction. Am J Obstet Gynecol. 212(1): 50. e1-8.