Previous Issues Volume 1, Issue 1 - 2017
Fibronectin as an Immunohistochemical Marker for Postmortem Diagnosis of Myocardial Infarction
Sepideh Saleki1, Farid Azmoudeh-Ardalan2*, Hamidreza Eftekhari2, Hayedeh Haeri2,Sahra Emamzadehfard2,3
1Legal Medicine Organization of Iran, Kahrizak, Tehran, Iran.
2Pathology Department, Imam Khomeini Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran.
3Radiology Department, University of Pennsylvania, Philadelphia, USA.
Corresponding Author: Farid Azmoudeh-Ardalan, Pathology department, Imam Khomeini Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran.
Tel: +98-912-1055232; E-Mail: [email protected]
Received Date: 13 Feb 2016
Accepted Date: 14 Mar 2016
Published Date: 22 Mar 2016
Copyright © 2016 Azmoudeh-Ardalan F
Citation: Azmoudeh-Ardalan F, Azmoudeh-Ardalan F, Eftekhari H, Haeri H, et al. (2016). Fibronectin as an Immunohistochemical Marker for Postmortem Diagnosis of Myocardial Infarction. M J Immu. 1(1): 001.
ABSTRACT
Acute myocardial infarction is sometimes a diagnostic dilemma in forensic pathology. Our aim is to evaluate the efficacy of fibronectin by immunohistochemical methods for diagnosis of early myocardial infarction in heart autopsies.Three groups of cases selected from autopsied hearts submitted to the pathology department of legal medicine organization of Iran during years 2004-2007 which included 15 cases of definite myocardial infarction (positive control group), 18 cases of noncardiac death (negative control group) and 26 cases suspicious of myocardial infarction based on clinical presentation just before death, presence of marked stenosis in at least one major coronary artery and exclusion of other causes of death (suspicious group). Fibronectin staining was performed on sections prepared from all of the cases. With our proposed cut off value for fibronectin staining the sensitivity and specificity of this marker are 93.3% and 94.4%, respectively. This marker could also support the occurrence of myocardial infarction in 42% of our suspicious cases.We conclude that in spite of usefulness of this marker for detection of myocardial infarction, the results should be interpreted with caution.
KEYWORDS
Myocardial Infarction; Fibronectin; Autopsy; Histopathology.
INTRODUCTION
Diagnosis of acute myocardial infarction is a challenging issue in forensic pathology. In autopsied hearts macroscopic findings of myocardial infarction accompanied by microscopic confirmation are the gold standards for diagnosis. However, the development of these changes requires time and in real practice we rarely are fortunate enough to see the typical cases. In most instances nothing other than significant narrowing of coronary arteries is found in favor of myocardial infarction. Use of an ancillary method is highly advocated in these situations. Application of triphenyltetrazolium chloride to the fresh myocardium, electron microscopy and some immunohistochemical markers including myoglobin, fatty acid binding protein (FABP), troponin, desmin, fibronectin, fibrinogen, C5b-9 and vascular endothelial growth factor (VEGF) are among many different diagnostic methods which have been used to address this diagnostic dilemma [1-10]. The electron microscopy is not available in every pathology laboratory and requires comprehensive expertise. The triphenyltetrazolium chloride method requires fresh tissue and a great deal of suspicion at the time of autopsy. The immunohistochemical studies are, however, promising alternatives. The aim of the current study is to evaluate the diagnostic power of one of these immunohistochemical markers, the fibronectin, in suspicious cases of myocardial infarction.
MATERIALS AND METHODS
Subjects
Three groups of autopsied hearts were used in this study as follows: 1. A group with definite evidence of myocardial infarction, the positive control group 2. A group with other causes of death unrelated to myocardium including accidents, electrical and thermal burns, and the negative control group 3. A group with strong clinical suspicion of myocardial infarction and presence of significant stenosis of coronary arteries (i.e. more than 75% stenosis of at least one of the three major coronary arteries), but without irrefutable macroscopic or microscopic evidence of myocardial infarction. Other causes of death were excluded in this group by comprehensive examination of the corpse, histopathologic evaluation of different organ systems and toxicological studies. Myocardial infarction is usually suggested as the cause of death in these circumstances. This group which is called the suspicious group in our study is the most challenging one in forensic pathology. The cases were selected from specimens submitted to the pathology department of legal medicine organization of Iran during years 2004-2007. Although it has previously been shown that even advanced putrefaction has no detrimental effect on fibronectin staining, cases with obvious putrefaction or autolysis were excluded from the study [11]. We examined at least one section from the macroscopically abnormal area in the positive control group, one section from the anterior wall of the left ventricle in the negative control group and at least three sections from the most vulnerable areas suggested by the location of the occluded coronary artery or arteries. From each section after routine processing two slides were prepared; one stained with H&E method and the other stained for fibronectinimmunohistochemically as stipulated below.
Immunohistochemical Staining
The autopsied hearts were fixed in 10% formalin and tissue sections processed routinely. The processed sections were embedded in paraffin block and from which 4 micrometerthick slide sections were prepared and transferred to sialinized microscopic slides. The slide sections incubated for one hour in 60˚C and then deparaffinized in two changes of xylene each for 5 minutes. Then the endogenous peroxidase activity was blocked by incubation for 15 minutes using 3% hydrogen peroxide in methanol. After washing with Tris-buffered saline (TBS), the slides were incubated for 35 minutes by the primary antibody (1/1000 dilution of a proprietary Rabbit anti human fibronectin, monoclonal antibody, Dakocytomation, Denmark). Next the unbound antibody was washed away by floating the slides in three changes of TBS, three minutes each. Finally, the potentially bounded antibodies were developed and detected by LSAB2 System-HRP detection kit (Dakocytomation, Denmark) according to the manufacturer's instructions.
Interpretation of IHC Study and Scoring System
Each slide was reviewed independently by two pathologists and scored in areas with the highest score based on the following system disregarding the dimensions of the stained area(s). All discrepancies in scoring between pathologists were then settled by simultaneous re-evaluation of slides:
0; No Staining (Figure 1)
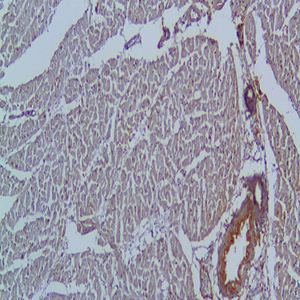
Figure 1: Mild cytoplamic staining in a suspicious case. The pattern of staining is patchy. This case was scored 1+. 100X
1+; Focal Weak Staining (Figure 2)
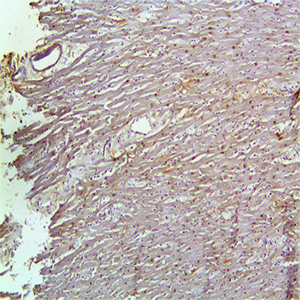
Figure 2: No staining for fibronectin expect for the blood vessel wall in a case of noncardiac death, negative control group (score=0). Blood vessel staining can be used as an internal positive control which supports correct staining procedure. 40X
2+; Intense Patchy Staining (Figure 3)
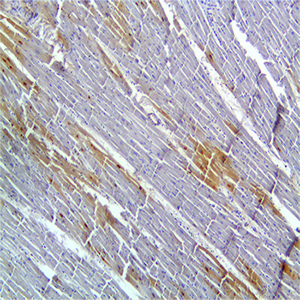
Figure 3: Patchy relatively strong nuclear and cytoplasmic staining in a case suspicious for myocardial infarction. This case was scored 2+. 100X
3+; intense diffuse staining (Figure 4)
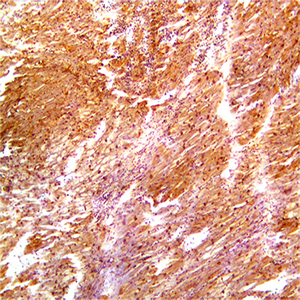
Figure 4: Strong confluent staining for fibronectin (Score=3+) at the site of infarction in a positive control subject. Marked polymorphonuclear leukocyte infiltration is also seen. 100X
Ethical Issues
The families of the deceased gave verbal consent for histopathological and toxicological studies. Additionally, no more expenses were imposed on the families for the IHC studies.
Statistical Analysis
SPSS version11.5 was used for statistical analysis. The mean of ages in different groups was compared by ANOVA and POSTHOC (Scheffe) tests. The sexes compared by the Chi square test. For comparison of fibronectin staining in different groups, Kruskal-Wallis and Mann-Whitney tests were used. P values less than 0.05 were considered significant.
RESULTS
The results of the study are summarized in Table 1.
| Groups | ||||
|---|---|---|---|---|
| Positive Control | Negative Control | Suspicious | ||
| Total number of cases | 15 | 18 | 26 | |
| Age (years)* | Mean | 53.73 | 36.11 | 47.65 |
| Standard Deviation | 14.533 | 14.212 | 12.093 | |
| Minimum | 30 | 14 | 25 | |
| Maximum | 75 | 56 | 76 | |
| Sex** | Male/Female | 12/3 | 17/1 | 24/2 |
| Fibronectin (scoring)*** | Negative | 0 | 13 | 6 |
| 1+ | 1 | 4 | 11 | |
| 2+ | 4 | 1 | 8 | |
| 3+ | 10 | 0 | 3 | |
| Mean Rank+ | 49.70 | 15.67 | 30.84 | |
DISCUSSION
Acute myocardial infarction is still a major cause of death in many parts of the world, especially in developing countries [12]. The correct diagnosis of myocardial infarction is of paramount importance in forensic science. Unfortunately, this diagnosis is not always easy due to the dearth of histopathological changes in some circumstances, e.g., dying soon after onset of clinical manifestations or occlusion of coronary vessels. To deal with this problem various diagnostic approaches have been proposed which run the gamut from simple histochemical methods to sophisticated procedures like electron microscopy [1-7]. Immunohistochemistry is a simple procedure which can be performed in most pathology laboratories and obviates the need for fresh tissue or sophisticated instruments. With advent of immunohistochemistry, many markers have been evaluated in this regard with promising results. These markers can be divided into those that are released from cardiomyocytes after ischemia and those that spill over into the site of ischemia and damaged cardiomyocytes from other sources like plasma and extracellular matrix. Troponin, FABP, Myoglobin and desmin are examples of the former and fibronectin, fibrinogen and C5b-9 belong to the latter. Fibronectin is a glycoprotein normally present in extracellular matrix and plasma with thrombotic, inflammatory, angiogenic and fibrogenic functions [9- 13]. With damage of cell membrane fibronectin runs into the cell in vital states and this property of which has been extensively utilized in forensic realm for confirmation of injuries taking place before death in trauma to skin, neck and skeletal muscle [9,14-17]. In our study we showed like other studies that intracellular fibronectin is directly connected with myocardial infarction. This marker stains large vascular channels as previously alluded to and this characteristic can be used as an internal control for ascertaining the acceptable quality of staining [7]. We have seen nuclear staining with or without cytoplasmic reaction in some cases. As this change frequently occurred in non-infarcted myocardium, i.e. negative control group, we disregarded this change and scoring was based solely on cytoplasmic staining (Figure 5).
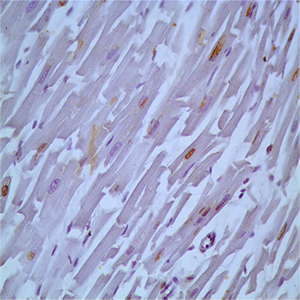
Figure 5: Strong nuclear staining in a negative control case. Note absence of cytoplasmic staining. 400X
The nuclear staining has been mentioned in another study [18]. In contrast to our study, authors of that study considered the nuclear staining as an evidence of myocardial infarction. Further studies are required to determine the significance of this change. Although fibronectin is more commonly and more intensely stained in myocardial infarction and despite its significance from the statistical point of view, slight overlap exists between the different groups precluding this marker from being impeccable for all problematic cases. Mild staining (1+) was seen in few negative control cases; even we had a moderate (2+) reaction in one case. These unexpected results suggest the possibility of wrong categorization of cases i.e. there may be some kind of myocardial injury in cases of unexpected positive result. C. Ortmann et al, have shown false positive results in cases with hypoxic changes just before death, e.g. hanging6. The possibility of suffocation cannot be excluded with certainty in some of our negative control cases, especially those perishing in vehicle accidents. Fibronectin staining was positive with variable intensity in all of our positive control cases as seen in other studies. However, the reaction was mild (1+) in one positive control case.Only in one study it has been shown that the intensity of staining may start fading from 3-7 days after occurrence of myocardial infarction9. These findings suggest that the results of this potentially valuable marker should be interpreted with cautious. As this marker is going to be a confirmatory test in suspicious cases, specificity is more important than sensitivity. These considerations and a trade-off between sensitivity and specificity are in favor of regarding negative and 1+ results as negative and 2+ and more as positive for myocardial infarction. With this cut-off value the sensitivity, specificity, positive predictive value and negative predictive value of this marker for diagnosis of myocardial infarction will be 93.3%, 94.4%, 93.3% and 94.4%, respectively. Considering this cutoff value, the fibronectin staining could confirm myocardial infarction in 42.3% of suspicious cases. We believe this is a reasonably good result, though not so encouraging as other studies have shown. In Hu's study, this marker could confirm myocardial infarction in 83.3% of suspicious cases7. This disparity may result from differences in procedures, types and dilutions of antibodies, populations, exclusion criteria and selection strategies. Some of the limitations of this study include; the limited number of female subjects, younger age of subjects in the negative group in comparison to the other two groups, not being aware of the exact time of death and elapsed time before performance of autopsy, the possibility of faulty categorization of cases i.e. some cases of genuine myocardial infarction at the time of an accident may be placed in the negative control group.
CONCLUSION
Although fibronectin is a very useful marker for detection of myocardial infarction, the results should be interpreted with caution. Probably, simultaneous application of two or more markers with different mechanisms of action such as troponin coupled with fibronectin will increase both the sensitivity and reliability of results. We suggest the performance of more human studies and evaluation of more markers preferably simultaneously. It is also highly advocated that each laboratory determines or at least confirms the specificity and sensitivity of immunohistochemical markers in their own settings before their implementation for postmortem diagnosis of myocardial infarction.
ACKNOWLEDGEMENT
Hereby the authors of the manuscript wish to thank all the personnel of pathology departments of Tehran University of Medical Sciences and Legal Medicine Organization of Iran for their sincere co-operation. This study is financed by a grant from Legal Medicine Organization of Iran.
REFERENCES
- Holmbom B, Naslund U, Eriksson A, Virtanen I, et al. (1993). Comparison of triphenyltetrazolium chloride (TTC) staining versus detection of fibronectin in experimental myocardial infarction. Histochemistry. 99(4), 265-275.
- Caulfield J and Klionsky B. (1959). Myocardial ischemia and early infarction: an electron microscopic study. Am J Pathol. 35(3), 489-523.
- Hansen SH and Rossen K. (1999). Evaluation of cardiac troponin I immunoreaction in autopsy hearts: a possible marker of early myocardial infarction. Forensic Sci Int. 99(3), 189-196.
- Ortmann C, Pfeiffer H and Brinkmann B. (2001). Immunohistochemical alterations after intravital and postmortem traumatic myocardial damage. Int J Legal Med. 115(1), 23-28.
- Xu XH, Chen JG and Zhu JZ. (2001). Primary study of vascular endothelial growth factor immunohistochemical staining in the diagnosis of early acute myocardial ischemia. Forensic Sci Int. 118(1), 11-14.
- Ortmann C, Pfeiffer H and Brinkmann B. (2000). A comparative study on the immunohistochemical detection of early myocardial damage. Int J Legal Med. 113(4), 215-220.
- Hu BJ, Chen YC and Zhu JZ. (1996).Immunohistochemical study of fibronectin for postmortem diagnosis of early myocardial infarction. Forensic Sci Int. 78(3), 209-217.
- Campobasso CP, Dell'Erba AS, Addante A, Zotti F, et al. (2008). Sudden cardiac death and myocardial ischemia indicators: a comparative study of four immunohistochemical markers. Am J Forensic Med Pathol. 29(2), 154-161.
- Casscells W, Kimura H, Sanchez JA, Yu ZX, et al. (1990). Immunohistochemical study of fibronectin in experimental myocardial infarction. Am J Pathol. 137(4), 801-810.
- Knowlton AA, Connelly CM, Romo GM, Mamuya W, et al. (1992). Rapid expression of fibronectin in the rabbit heart after myocardial infarction with and without reperfusion. J Clin Invest. 89(4), 1060-1068.
- Ortmann C, Pfeiffer H and Brinkmann B. (2000). Demonstration of myocardial necrosis in the presence of advanced putrefaction. Int J Legal Med. 114(1-2), 50-55.
- Boersma E, Mercado N, Poldermans D, Gardien M, et al. (2003). Acute myocardial infarction. Lancet. 361, 847-58.
- Orem C, Celik S, Orem A, Calapoglu M, et al. (2002). Increased plasma fibronectin levels in patients with acute myocardial infarction complicated with left ventricular thrombus. Thromb Res. 105(1), 37-41.
- Fieguth A, Franz D, Lessig R and Kleemann WJ. (2003). Fatal trauma to the neck: immunohistochemical study of local injuries. Forensic Sci Int. 135(3), 218-225.
- Fieguth A, Kleemann WJ, von Wasielewski R, Werner M, et al. (1997). Influence of postmortem changes on immunohistochemical reactions in skin. Int J Legal Med. 110(1), 18-21.
- Grellner W, Dimmeler S and Madea B. (1998). Immunohistochemical detection of fibronectin in postmortem incised wounds of porcine skin. Forensic Sci Int. 97(2-3), 109- 116.
- Fechner G, Bajanowski T and Brinkmann B. (1993). Immunohistochemical alterations after muscle trauma. Int J Legal Med. 105(4), 203-207.
- van Dijk A, Niessen HW, Ursem W, Twisk JW, et al. (2008) .Accumulation of fibronectin in the heart after myocardial infarction: a putative stimulator of adhesion and proliferation of adipose-derived stem cells. Cell Tissue Res. 332(2), 289- 298.