Previous Issues Volume 3, Issue 1 - 2018
Efficacy of the Supramaximal Technique in the Correction of Palpebral ptosis. Randomized Surgical Trial
C. María Cáceres Toledo1,Odalys Cáceres Toledo2,María Eva Saavedra Saavedra3
1Second Degree Specialist in Ophthalmology. Doctor of Medical Sciences. Professor and Principal Investigator.
2First Degree Specialist in Ophthalmology and MGI. Assistant Professor.
3nd MGI. Assistant Professor.
Corresponding Author: María Cáceres Toledo, Second Degree Specialist in Ophthalmology. Doctor of Medical Sciences. Professor and Principal Investigator, Cuba, E-Mail: [email protected]
Received Date: 07 Sep 2018 Accepted Date: 14 Sep 2018 Published Date: 18 Sep 2018 Copyright © 2018 Toledo MC
Citation: Toledo MC, Toledo OC and Saavedra MES. (2018) Efficacy of the Supramaximal Technique in the Correction of Palpebral Ptosis. Randomized Surgical trial. Mathews J Ophthalmol 3(1): 020.
Introduction: The palpebral ptosis is defined as the fall of higher eyelid. According the millimeters of this type of fall it is classified in slight, moderate and severe.
Objective: To assess the effectiveness of the Supramaximal technique in the repair of moderate and severe palpebral ptosis.
Material and Methods: 95 patients were studied in a first cut, receiving treatment with the Supramaximal or Suspension to frontal. To determine the therapeutically effectiveness a simple-blind randomized clinical trial was made. The effectiveness was assessed as regards fall of high eyelid, height of palpebral fold, distance of border reflex and satisfaction of the patient. Results: The mean age was of 59, 35 years old. There was an average of female sex and of white race. The 51.6% of study patients have a severe ptosis. The therapeutically effectiveness of the Supramaximal was higher to Suspension to frontal (96.7% y 86.2%) respectively
Conclusions : The Supramaximal as a surgical technique is more efficacious than the Suspension one to frontal in the correction of moderate and severe higher palpebral ptosis.
Ptosis; Supramaximal; Suspension to frontal; Therapeutically Effectiveness.
INTRODUCTION
The Ptosis or drooping of the eyelid, constitutes a health problem, from the antiquity until our days, due to the affectation that it causes on the vision, and the facial aesthetics, mainly in the women, which predominate in almost all the published series [1-13].
The treatment of ptosis is surgical. Several techniques have been used for their correction, which go back to ancient times. Egyptian doctors burned the skin of the upper eyelid with hot gold plates so that the scar retraction would elevate it [1-3]. In modernity and with the introduction of technological advances such as the surgical microscope and the cutting and coagulation equipment, new techniques have been used with good results, among them the Supramaxim [1, 2-12].
Suspension to frontal with autologous fascia lata, has been the most used technique in moderate and severe palpebral ptosis, reason why it is considered the golden rule in its surgical correction [4, 5, 13].
However, for its realization a graft is required, which replaces the physiological mechanism of the palpebral opening and is not without complications.
It is considered that Supramaxim is a therapeutic alternative for cases with poor EPS function, which avoids the risk of infection and extrusion of the graft, does not require the extraction of the fascia lata, so it eliminates a scar and decreases the surgical time [1-13].
In the reviewed literature, the therapeutic results obtained with one or other of these techniques are known separately [1-3, 8-12] but until now, no study has been published to determine which is the most effective. The above is a controversial issue not yet resolved by the scientific community.
In the present investigation, a randomized clinical trial has been designed to demonstrate the aforementioned.
The main objective is: To evaluate the efficacy of the supramaximal surgical technique in the correction of moderate and severe upper palpebral ptosis.
METHODOLOGICAL DESIGN
A simple blind randomized surgical trial was performed, in which patients from the outpatient clinic of Ophthalmology of the Hermanos Ameijeiras Hospital (HHA) participated. It was carried out from February 2016 to November of the year 2017.
UNIVERSE. All patients with palpebral ptosis of moderate to severe and who meet the selection criteria.
Only cases with this type of ptosis are selected, because both techniques are indicated in their surgical correction. SAMPLE. It was calculated by the CTM program version 1.1 (See Annex 1).
Patients who attended the Neurophthalmology clinic of the HHA, from February 2016 to November 2017, who met the selection criteria were included. The assignment to each treatment group was carried out randomly and blindly, because it is not possible to“pick up” the surgeon, because of the evidence that the wounds represent, on the patient’s forehead, in one of the techniques.
The sample was composed of 95 patients, 48 were performed Supramáxima technique and 47 suspension to the frontal.
Inclusion criteria. Patients over 18 years of age, with moderate and severe upper palpebral ptosis.
Exclusion criteria. Patients with dry eye, in the decompensated of systemic diseases such as Diabetes Mellitus and Myasthenia Gravis. Patients with ptosis of mechanical cause due to allergic conjunctivitis and tumors.
The ophthalmological examination was performed, the measurement of the EPS muscle function, the palpebral fissure and the DMR. The degree of clinical involvement of ptosis (moderate or severe) was based on the classification of Salcedo et al [1]. The data obtained will be recorded in the data dump template.
OPER OPERATION OF THE VARIABLES
Main response variable Combined results Satisfactory When after the surgical techniques used in the patients decrease the millimeters (mm) or return to the palpebral physiological level with respect to the preoperative values of the following variables: upper eyelid drop, margin-reflex distance (DMR), height of the fold palpebral orbital and in which the satisfaction of the patient is obtained.
Not satisfactory When after the surgical techniques used in the patients do not improve one or more of the above-mentioned parameters and the patient’s dissatisfaction.
DESCRIPTION OF SURGICAL TECHNIQUES
Surgical TechniqueSupra Máxima By cutaneous route access to the aponeurosis of the elevator until reaching the “Whitnall” ligament which is fixed to the tarsus with nonabsorbable suture, the height of the eyelid is checked and the skin is sutured
Surgical Technique Frontal Suspension with Fascia Autologous can In the frontal region at supraciliary level 3 incisions of 5 mm are made. In the tarsus the fascia lata is fixed with absorbable suture, and its ends are directed by means of the fascia needle towards the previously made incisions, crossing the muscles: orbicular and frontal, both are joined and knotted in the medial incision. The eyelid height is checked and the skin is sutured.
The data was processed using the Epidat 3.1 and SPSS version 20 programs. The Chi-square test was applied to find differences between the results of both techniques. The Relative Risk was calculated with the 95% confidence interval.
ETHICAL ASPECTS
The Universal Declaration on Bioethics and Human Rights (2005) [16] was complied with and with the current legislation in Cuba, in accordance with the provisions of the National Health System, established in Law No.41.
RESULTS
In the series studied, the average age was 59.35 years. There was a predominance of female sex (56.8%) and white skin (75.8%). 51.6 %% of the patients studied have severe ptosis.
Table 1 shows the results combined with both techniques. They were satisfactory in 91.5% of the patients, with a higher percentage in the Supramaxim technique compared to the frontal suspension: 96.7% and 86.2% respectively, however the difference between the two was not significant (p = 0.051).
Table 1: Therapeutic efficacy according to groups and combined results. Average of operated eyes.
| Combined results | Supramaximum | Suspension to the frontal | Total | Significance(p) |
| Satisfactory | 58 (96.7%) | 50 (86.2%) | 108(91.5%) | 0.051* |
| Not Satisfactory | 2 (3.3%) | 8 (13.8%) | 10 (8.5%) | |
| Total | 60 | 59 | 119 |
*Chi square test
Table 2: Therapeutic efficacy according to groups and related variables.
| Variables | Supramaximum | Suspension to the frontal | Total | Significance(p)* |
| Upper eyelid droop | ||||
| satisfactory | 60 (100.0%) | 51 (87.9%) | 111(93.3%) | 0.006* |
| Not Satisfactory | 0 (0.0%) | 8 (13.8%) | 8 (6.7%) | |
| Reflection margin distance | ||||
| satisfactory | 59 (98.3%) | 52 (88.1%) | 111(93.3%) | 0.032* |
| Not Satisfactory | 1 (1.7%) | 7 (11.9%) | 8 (6.7%) | |
| Height of the orbito-palpebral fold | ||||
| satisfactory | 59 (98.3%) | 51 (87.9%) | 110(93.2%) | 0.031* |
| Not Satisfactory | 1 (1.7%) | 8 (13.8%) | 9 (7.6%) | |
| Eyelid clef | ||||
| satisfactory | 59 (98.3%) | 52 (88.1%) | 111(93.3%) | 0.032* |
| Not Satisfactory | 1 (1.7%) | 7 (11.9%) | 8 (6.7%) | |
| Muscle function | ||||
| satisfactory | 59 (98.3%) | 51 (87.9%) | 110(93.2%) | 0.031* |
| Not Satisfactory | 1 (1.7%) | 8 (13.8%) | 9 (7.6%) | |
| Total | 60 | 59 | 119 | |
Table 2 shows that the correction of upper eyelid drooping and reflex margin distance was satisfactory in all patients in whom the Supramaxim technique was used. This result was significantly greater with respect to the frontal suspension, (p = 0.006).
The height of the orbito-palpebral fold, the palpebral fissure and the function of the levator palpebrae superior muscle were also satisfactory in a significantly higher percentage with the Supramaxim technique.
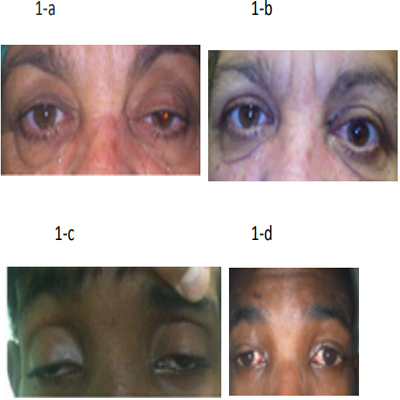
Figure 1: Surgical results with both techniques. Before and after surgery 1-a and 1-b with the Supramaxim, 1-c and 1-d with the Suspension to the Frontal.
Table 3 shows the degree of satisfaction, which was higher with the Supramaxim (97.9%), but the difference between the two was not significant (p = 0.111).
Table 3: Therapeutic efficacy according to groups and patient satisfaction.
| Patient satisfaction | Supramaximum | Suspension to the frontal | Total | Significance(p) |
| satisfactory | 47 (97.9%) | 42 (89.4%) | 89 (93.7%) | 0.111* |
| Not Satisfactory | 1 (2.1%) | 5 (10.6%) | 6 (6.3%) | |
| Total | 48 | 47 | 95 |
* Chi square test
DISCUSSION
Most authors agree that the most used techniques for moderate and severe palpebral ptosis are the Suspension to the frontal and the Supramaxim [1-13, 16-18].
With the Supramaxim surgical technique, a greater percentage of satisfactory results was achieved compared to the frontal suspension. Similar results have been reported by other authors, [5-12] which consider that with the Supramaxim the action of the EPS is reinforced and the physiological mechanism of ocular opening is conserved, however, with the Suspension to the Frontal, this mechanism is replaced by a tissue inserted between the tarsus and the frontal muscle.
In the e Cáceres and cols 7 series, excellent therapeutic results were obtained with the frontal suspension with autologous fascia lata and in the two cases operated with the maximum reinforcement of the EPS.
Negrin-e Cáceres et al [12] have obtained similar results with Supramaxim in 95 operated cases.
In the report by Nagaraju et al, [10] both techniques were compared. The frontal suspension was performed at 60% of the eyes and the Supramaxim on the remaining 40%. Optimal correction was achieved in 56% of the patients without significant differences between the two comparison groups.
In Japan, [18] good results have been reported with frontal suspension surgery, since all patients achieved satisfactory functional results. In a study carried out in China, [18] satisfactory results were obtained in 92% of the 55 patients (75 eyes) operated on with the Frontal Suspension technique with severe congenital ptosis. These results exceed those achieved in the present. clinical trial; However,Gómez et al [18] report an 81% success rate with the same technique, which is lower than that obtained for the two techniques evaluated in our trial.
In studies conducted in Cuba, Jerez et al, [18] managed to correct 29 eyes (87.87%) with the Suspension to the frontal and although three cases were hypocorrected, it was suggested that the surgical technique was satisfactory, as they were mostly null or poor excursion of the eyelid lift muscle.
Patient satisfaction was achieved with both techniques, although it was higher in Supramaxim. This parameter is closely related to the quality of life, which is a pillar of medicine in Cuba. In the literature consulted [1-18], no data are collected that assess the post-operative satisfaction of patients with eyelid ptosis, which reinforces the aforementioned.
REFERENCES
- Salcedo Casillas G. (2001). Periorbital cosmetic surgery. Anatomical bases of palpebral aesthetics. Upper eyelid. Upper palpebral groove. Mexico. DF: Association to prevent blindness in Mexico. 87-96.
- Goldberg RA and Lew H. (2011). Cosmetic outcome of posterior approach ptosis surgery (American Ophthalmological Society Thesis). Trans Am Ophtalmol Soc. 109: 157-167.
- Malhatra R, Salam A, Then SY and Grieve AP. (2011). Visible iris sign as a predictor of problems during and following anterior approach ptosis surgery. Eye. 25(2): 185-191.
- Gundeslioglu AO, Selimoglu MN and Bekerecioglu M. (2013). A frontalis sling operation using an autogenous en-bloc, fan-shaped tensor fascia lata graft for blepharoptosis. J Plast Reconstr Aesthet Surg. 66(2): 224-230.
- Nakauchi K, Mito H and Mimura O. (2013). Frontal suspension for congenital ptosis using an expanded polytetrafluoroethylene (Gore-Tex(®)) sheet: one-year follow-up. Clin Ophthalmol. 7: 131-136.
- Cáceres M, Ponce Y and Linares D. (2008). Abordaje anterior versus posterior en la corrección de la Ptosis palpebral. Rev Cubana Oftalmolog.
- Cáceres M, Cáceres O, Fresneda J and Márquez M. (2016). Aplicaciones del Gore-tex en Oftalmología. Rev. Cubana Oftalmolog. 27(1).
- Jung Y and La TY. (2013). Blepharoptosis Repair through the Small Orbital Septum Incision and Minimal Dissection Technique in Patients with Coexisting Dermatochalasis. Korean J Ophthalmol. 27(1): 1-6.
- Jung Y and La TY. (2013). Blepharoptosis Repair through the Small Orbital Septum Incision and Minimal Dissection Technique in Patients with Coexisting Dermatochalasis. Korean J Ophthalmol. 27(1): 1-6.
- Gundeslioglu AO, Selimoglu MN and Bekerecioglu M. (2013). A frontalis sling operation using an autogenous en-bloc, fan-shaped tensor fascia lata graft for blepharoptosis. J Plast Reconstr Aesthet Surg. 66(2): 224-230.
- Gundeslioglu AO, Selimoglu MN and Bekerecioglu M. (2013). A frontalis sling operation using an autogenous en-bloc, fan-shaped tensor fascia lata graft for blepharoptosis. J Plast Reconstr Aesthet Surg. 66(2): 224-230.
- Matayoshi S, Cardoso I and Rossato L. (2014). Surgical treatment of congenital blepharoptosis. Rev. bras.oftalmol. 73(4).
- Nagaraju G, Muthu S, Chinmayee JT and Kailash PC. (2015). Evaluation of outcome of Various Surgical Procedures for Upper Eyelid Ptosis. Journal of Evidence based Medicine and Healthcare. 2(9): 1180-1187.
- (2005). Declaración Universal sobre Bioética y Derechos Humanos. 33 Sesión Conferencia General de la UNESCO: 917-924
- Hashem AM, Couto RA, Waltzman JT, Drake RL, et al. (2017). Evidence-Based Medicine: A Graded Approach to Lower Lid Blepharoplasty. Plast Reconstr Surg. 139(1): 139e-150e.
- Wang CY. (2013). Treatment of severe congenital ptosis by frontal muscle flap suspension surgery. Guoji Yanke Zazhi (Int Eye Sci). 13(1): 175-176.
- Gómez Cabrera CG, Ramírez García LK and Rojas Rondón I. (2014). Técnica de Crawford en el tratamiento de la ptosis palpebral congénita. Rev Cubana Oftalmol. 27(1).
- Jerez EFP, Ramón Reyes E, Ortuño Águila DM, Fernández YEA, et al. (2015). Frontal suspension technique in the correction of palpebral ptosis. Multimed. 19(5).
- Gundeslioglu AO, Selimoglu MN and Bekerecioglu M. (2013). An frontalis sling operation using an autogenous en-bloc, fan-shaped tensor fascia lata graft for blepharoptosis. J Plast Reconstr Aesthet Surg. 224-230.
- Cagatay HH, Ekinci M, Apil A, Arslan B, et al. (2014). The Use of Polypropylene Suture as a Frontalis Suspension Material in All Age Groups of Ptosis Patients. Journal of Investigative Surgery. 240-244.