Previous Issues Volume 3, Issue 1 - 2018
Effects of Art Experience on Hospitalized Pediatric Patients
Frances K. Lopez-Bushnell*1 , Marian Berg2
1Director of Nursing Research, University of New Mexico Hospital, Albuquerque, New Mexico.
2Artist and nurse at the University of New Mexico Hospital, Albuquerque, New Mexico.
Corresponding Author: Lopez-Bushnell FK, Director of Nursing Research, University of New Mexico Hospital, Albuquerque, New Mexico, E-Mail: [email protected]
Received Date: 10 Jul 2018 Accepted Date: 16 Jul 2018 Published Date: 20 Jul 2018
Copyright © 2018 Lopez-Bushnell FK
Citation: Lopez-Bushnell FK and Berg M. (2018). Effects of Art Experience on Hospitalized Pediatric Patients. Mathews J Pediatr. 3(1): 013.
ABSTRACT
This is an IRB approved randomized pre/post control trial that measured the effect of art making and creative experiences on the vital signs of hospitalized children Children who are hospitalized for long periods of time are often isolated and lonely, which may result in increased stress levels and depression. Many parents and family relatives cannot visit these children due to work and family responsibilities. The objectives of this research were to measure how art making activities may be helpful in providing a way for children to express themselves, induce relaxation and reduce stress responses (lower heart rate and increase oxygen saturation) and improve psychological and physiological well-being of children in hospital settings. Research findings demonstrated that art can support stress reduction.
The hypothesis was that when an art facilitator provided children with art materials and prompts at the bedside and engaged them in art making, their stress levels would decrease. Stress levels were measured by monitoring the heart rate and oxygen saturation before and after the activity for those patients on monitors. Emotional affect and pain level were also assessed using the Wong-Baker Pain Scale. This study was conducted in the UNMH General Pediatrics Unit and the Pediatric Specialty Care Unit.
KEYWORDS
Hospitalized Pediatric Patients; Art Experience; Vital Signs.
INTRODUCTION
The General Pediatric Unit (GPU) at UNM Children's Hospital currently has 28 private rooms and 4 double occupancy rooms for a total of 36 patient beds. The GPU is an inpatient area that cares for patients from infancy to seventeen years of age. The patient population consists of individuals experiencing respiratory illness, dehydration, burns, trauma, surgical and orthopedic issues as well as patients with chronic diseases including renal failure, gastrointestinal disease, cystic fibrosis, asthma and neurological impairments. GPU is a step-down unit for the Pediatric Intensive Care Unit and admits patients from multiple areas within the UNM hospital system such as clinics, surgery, urgent care, emergency room, and other inpatient units, as well as patients from throughout New Mexico and surrounding states. The Pediatric Specialty Care Unit (PSCU) holds 20 beds, with most patients suffering from renal, oncological, and immune deficiency diseases. On both of the pediatric units, the number of patients that reside in isolation rooms can span from 10% to 70%. All of the rooms on both units have central monitoring capabilities, however, not all of the patients are on monitors.
LITERATURE REVIEW
The literature review indicated that art is therapeutic and beneficial for hospitalized children. In her article, "Medical Art Therapy with Children", Councill (2003) found that children in a medical setting, who participated in creative works, increased their sense of hope, autonomy, competence and self esteem in the children. Participation in art also facilitated the safe and contained expression of feelings in the child. Malchiodi (1999) described how art therapists, nurses, counselors, psychologists, and play therapists, among many others, used art expression therapeutically in hospitals. She defined medical art therapy as "the use of art expression and imagery with individuals who are physically ill, experiencing trauma to the body, or who are undergoing aggressive medical treatment such as surgery or chemotherapy" (p. 66).
Sundaram (1998), an art therapist, did a case study of a sevenyear-old male who had been hospitalized for a fractured leg. She worked with him for six one-hour sessions over a twoweek period. Her goal for his therapy was threefold: to give him an outlet for his feelings regarding hospitalization, to enable him to have a feeling of control over his environment, and to provide stimuli to decrease his anxiety about being hospitalized. She concluded that the combination of art and play was successful in facilitating the therapeutic process. This dual process helped the child express himself, achieve increased awareness of himself, and helped to internally process the impact of the injury or illness.
Koller (2008) defines therapeutic play as specialized activities that facilitate emotional well-being and are developmentally supportive of the pediatric patient. Therapeutic play helps the child cope with difficult situations such as hospitalization or other medical experiences. Therapeutic play can be combined with expressive arts to elicit emotional expression and decrease anxiety and fear in the hospitalized child.
Yount, Rachlin and Sieglel (2013) studied the effects of art therapy on 25 pediatric patients. In the article, "Expressive arts therapy for hospitalized children", they described how there was a measurable decrease in patient's salivary cortisol levels following the making of "Healing Sock Creatures" Saliva samples were collected before and after the creative experiences. This is one of the first studies that measured a biomarker of stress following an expressive art therapy session.
Dionigi and Gremigni (2016) studied how a combined intervention of art therapy and clown visits would enhance the efficacy of anxiety-reducing oral medication in children prior to anesthesia induction and surgery. All 78 children in the study received Midazolam 30 minutes prior to surgery. The control group underwent general anesthesia per standard practice and the intervention group received art therapy and clown visits prior to surgery. Children in the intervention group showed a significant reduction in the Modified Yale Preoperative Anxiety Scale at parental separation compared with the control group. The study concluded that the art therapy and clown intervention enhanced the effect of Midazolam and decreased the children's anxiety during the preoperative separation from parents.
Rollins, Drescher and Kelleher studied how using an artist to draw by proxy intervention helped improve the quality of life for hospitalized children. Their research study utilized an artist that drew images suggested by the children to help the children articulate their feelings. The book, "Moon Balloon, a Journey of Hope and Discovery for Children and Families", written by one of the researchers, Fran Drescher, was used as a basis for this quantitative/qualitative research study. The authors concluded that the "Moon Balloon" intervention was effective in helping children express their feelings about hospitalization, illness and other issues.
Wallace, Packman, Huffman, et al studied the effects of the pediatric hematopoietic stem cell transplant (HSCT) procedure on the siblings of transplant recipients. The siblings engaged in timed series of three art therapy sessions at specific intervals following their family member's HSCT treatment. The intervention group showed improvement in psychosocial functioning and lowered levels of posttraumatic stress symptoms compared to the control group.
A study undertaken at a Swedish hospital (Wikstrom, 2005) investigated how children used expressive art mediums in a play therapy unit. At this hospital, children could visit the play therapy unit anytime during the day and were given a choice of what art medium they want to work with (clay, paint, textiles, etc.). Researchers noted that emotional pain may manifest as crying, decreased communication, and insomnia in the hospitalized child. Some children also exhibit regression in their growth and development as a result of the stress of hospitalization. The main finding in this study was that the children were able to express emotions such as fear and powerlessness through their art. "The crucial point in their activities was when they transformed their reality through the expressive art activity they had chosen. They reshaped their world after their own needs, and found satisfaction through the symbolic, expressive art activities" (Wikstrom, 2005). The study, published in a pediatric nursing journal, concluded that expressive arts were a valuable way for the children to communicate feelings that they might not have been able to express verbally.
The practices of visualization techniques, positive thinking, and expressive arts to activate the immune system are becoming more widespread and accepted in the medical world. (Malchiodi, 1999). Some health professionals use art as a means of developing rapport with patients and a deeper communication about their illnesses. Surgeon Bernie Siegel (1999) asked his patients to make simple drawings as a way of initiating dialogue about feelings or experiences they might not share otherwise. Siegel discusses how his patient's drawings relate to Jung and dream symbolism. He also writes about positive visualization techniques used by his patients for dealing with cancer and other illnesses.
Carol DeLue (1999) described how making mandalas has been shown to reduce stress and anxiety in children. She used biofeedback devices to measure children's peripheral temperature and heart rate before and after making mandala drawings. The results of the study indicated that, in contrast with the control group, significant relaxation was seen in children who had made mandalas. Carl Jung asserted that mandalas have "a calming and centering effect upon its maker" (DeLue, p. 47). This study verified that art making can facilitate a reduction of autonomic arousal and initiate a relaxation response.
ARTS-IN-MEDICINE
In the past forty years, the medical field has become more welcoming to the connection between medical treatment and the arts, resulting in the Arts-in-Medicine field. This new field recognizes the power of the arts to facilitate healing through creative self-expression. Creative encounters can encourage reflection and patient-centered behavioral change, create new perspectives and increase meaning in life, facilitate positive experiences and heighten self-esteem, stimulate a spiritual connection, provide opportunities for expression of painful and/or suppressed feelings, and relieve discomfort, including pain, anxiety/restlessness, respiratory difficulty, nausea, insomnia, isolation, depression and withdrawal. These art programs vary in purpose and design. Some programs emphasize patient interaction, such as art making at the bedside or in groups. Other programs set up art exhibits or employ local musicians to perform for patients and their families, all with the goal of humanizing the medical environment. The first hospital arts program in the U.S. began at Duke University Hospital in 1978 (Palmer and Nash, 1991). There are now approximately 1,000 hospital-based arts programs in various forms around the United States. The Arts-in-Medicine program at the University of New Mexico began in 2002 and has developed into a large program of complementary care serving approximately 30,000 patients, family members and staff per year in the main hospital, Children's Hospital, Carrie Tingley Hospital, UNM Psychiatric Hospital, UNM Cancer Center and various outpatient clinics.
In an article in the Arts and Health journal, Paul Sznewajs (2009) described his organization, the Snow City Arts Foundation in Chicago. This group has provided arts programs in Chicago pediatric wards since 1998. Most hospital-based pediatric art programs are based on either recreation or art therapy. Snow City is unique
in that it focuses on learning. The program arose as a response to the fact that chronically ill children often miss large amounts of classroom education. Sznewajs cited a study that indicated 103,000 school-aged children in Illinois annually missed extended amounts of school in 2003 due to illness (2007). Snow City Arts (SCA) has partnered with the city's public school system as well as local artists, universities, and cultural institutions to provide art-related educational opportunities for approximately fifteen hundred hospitalized children per year. SCA was founded in 1998 and employs nine Artists-inResidence in four Chicago hospitals. It works closely with Child Life services and the hospital staff and includes four separate educational workshops: creative writing, music, theater and visual arts. Partnership with the Chicago Public School system has enabled participants to receive classroom credit for work done in the hospital. National and state learning standards are integrated into the arts workshop evaluation systems so the curriculum is comparable to that taught in the classroom.
Rode (1995) discussed the interface of art therapy and child life programming. She is both a registered art therapist and a child life specialist. She wrote that the two parallel disciplines can collaborate working toward optimal adjustment for patients and their families by using play and the creative arts. Both the child life specialist and the art therapist function as translators of experience for the pediatric patients. They both look for play or art modalities that stimulate the children's imagination and foster a safe transitional space. In this space, through creative expression, the children can create a dialogue between the inner experience of illness (the pain, fears and fantasies) and the outer reality of the children's lives. Using play as the "mediating activity", the art therapist can assist the hospitalized children to explore images which "describe or respond to their illness". To give the experience a shape or form helps the children cope with their illness and prevents them from "falling into it" (p. 109). Both art therapists and child life specialists can attend to the imaginative lives of children.
This review of related literature suggests that art is therapeutic and beneficial for hospitalized children. Additionally, art therapy and art education have been successfully integrated into some hospital programs for children and adult patients. Arts-in-Medicine, although not a formal therapy, provides significant therapeutic benefits through the facilitation of art, music, dance, creative writing and drama activities.
STUDY DESIGN
This was a pediatric clinical pre/post study that measured hospitalized children's pain and emotion using the "WongBaker FACES Pain Rating Scale", and when the children were on monitors, the heart rate and oxygen saturation level were recorded before and after the art activity. The Parents or Legalized Authority Representative of the child signed a consent form giving permission to use the child's art for publication, although there were no identifiers collected. Depending on age, the child signed an assent form to give permission. The Child Life staff screened the inpatients in the General Pediatrics and Pediatric Specialty Care units and gave the names to the Art Facilitator.
The primary endpoints were the differences in the participant's oxygen saturation, heart rate, and pain responses before and after the art experience. The secondary, exploratory endpoints were the children's art creations and their interpretations of the art. Children whose parents did not sign the consent form were not included in the study, although they received the art experience if they wanted to participate. 200 participants from the General Pediatric Unit and the Pediatric Specialty Care Unit were included in this study, with 100 in the control group and 100 in the intervention group. Using 200 subjects with a T-Test Power Analysis (two groups), the effect size was .2 (small) with a significant level of .05 and a power of .804 with a df = 199, critical t = 1.972 and a non-centrality parameter = 2.828. The duration of an individual subject's participation in the research was 30 to 60 minutes. The study took approximately two years to complete. The safety endpoints were any critical vital sign changes or pain measurements which were reported to the primary nurse and physician immediately. The art facilitator was also a Registered Nurse with several years of experience who could identify any safety issues with the participants. The research team was given access to the subjects from the Child Life staff or nurses on the unit.
The only direct identifiers were the first names of the subjects and their locations. Personal health information was not known by the researchers unless volunteered by the family members and was not included in the data.
STUDY PROCEDURES
The research procedures were performed as follows
- Once consent had been obtained, the pediatric patient was asked what kind of art he/she would like to do. Heart rate and oxygen saturation levels indicated on the monitor were entered into the research log. Pain levels, if present, were obtained from the child.
- The child participated in the art activity.
- After approximately 20 minutes, the monitor recordings of heart rate and oxygen saturation were recorded and entered into the research log.
- The child was asked his/her opinion of the art creation and what it meant to him/her. This information was then entered into the research log. Pain levels were obtained from the child.
- Each child was given a code number so that there would be no identifiers related to the vital signs, the Wong Baker Scores, or any child's interpretation of the art project.
RECRUITMENT METHODS
All 200 subjects were recruited at the General Pediatric Unit and the Pediatric Specialty Care Unit. The list of patients was compiled by the Child Life specialist and given to the art facilitator on a weekly basis. No diagnosis or personal health information was given, only first names and ages of patients and their location. The control group was composed of children on monitors who either refused art activity or were not offered the activity due to time or other constraints. Heart rate and oxygen saturation were obtained at baseline and approximately 20 minutes after the baseline.
DATA ANALYSIS
An ANOV was used to measure the vital signs and Wong Backer scores before and after the art intervention. Using 200 subjects with a T-Test Power Analysis (two groups), the effect size was .2 (small) with a significant level of .05 and a power of .804 with a df = 199, critical t = 1.972 and a noncentrality parameter = 2.828.
Examples of Children's Artwork
For hospitalized children, making art is one of few empowering activities available to them when everything else seems out of their control.

This painting was done by an 18-year-old girl in the Specialty Unit. Her heart rate before the art activity was 77, and after was 78. Oxygen saturation before the art was 94%, and after was 96%.

This was painted by a 7-year-old girl with special needs. Her heart rate prior to the activity was 110, after was 86. Oxygen saturation before the activity was 87%, afterwards 93%.

The painting below was done by a 16 year old girl with special needs. She was visually impaired, and could only see in her peripheral visual field. Oxygen saturation before activity: 94%, after: 98%. Heart rate before the activity: 59, after: 58.

This was painted by a 6-year-old girl on Contact and Droplet precautions. She suctioned herself frequently with a long suction tube called "Mr.Thirsty". Oxygen saturation prior to the art activity was 97%, heart rate 135. After activity, oxygen saturation went up to 99, heart rate 89.

This 11-year-old boy was on contact and droplet precautions for a contagious respiratory illness. Prior to art making activity, his oxygen saturation was 87%, his heart rate was 123. Afterwards, oxygen saturation was 90%, heart rate 100.

This 7-year-old girl wanted to do a self-portrait. She was confined to her room in Contact and Droplet Precautions for a serious respiratory illness. When I came into the room, her affect was flat, heart rate was 104, oxygen saturation was 91%. After the activity, she seemed very proud of herself and her painting. Her heart rate decreased to 100, oxygen saturation increased to 95%.

This is a painting was done by an 11-year-old girl. Her heart rate prior to activity was 105, after 103. Oxygen saturation remained the same at 86%.

This was done by a 9-year-old male who underwent abdominal surgery earlier in the day. I asked him what his favorite superhero was and he chose to paint Iron Man. Oxygen saturation prior to activity was 88%, afterwards went up to 91%. Heart rate prior to activity was 91, then decreased to 80.

This pink monkey was painted by an 8-year-old girl.
Her heartrate was 104 prior to the activity, and her oxygen saturation was 97%. She was very enthusiastic and excited during the activity, and her heart rate increased to 120. Oxygen saturation also increased to 99.
These paintings were done by a 6-year-old who was in Contact and Droplet precautions for a contagious respiratory illness. She was on oxygen via mask and had an IV. She was speech impaired, developmentally delayed and alone in her room. Her heart rate prior to the activity was 140, afterwards, 134. Oxygen saturation before the art making activity was 87%, after was 90%.

This 7-year-old girl was on oxygen and had an IV in her dominant right hand, so she had to use her left hand to paint. Prior to the activity, her affect was flat, pulse 110, oxygen saturation 95%. As she painted, her affect brightened, her pulse decreased to 106 and her oxygen saturation increased to 96%.
On the evaluation paper, her mother indicated that "the child felt" "great" after doing activity

The 8-year-old girl who painted the picture above passed away shortly before this article was written. She had been hospitalized frequently over a long period of time. Most likely, the artwork the children leave behind is very precious for their families.

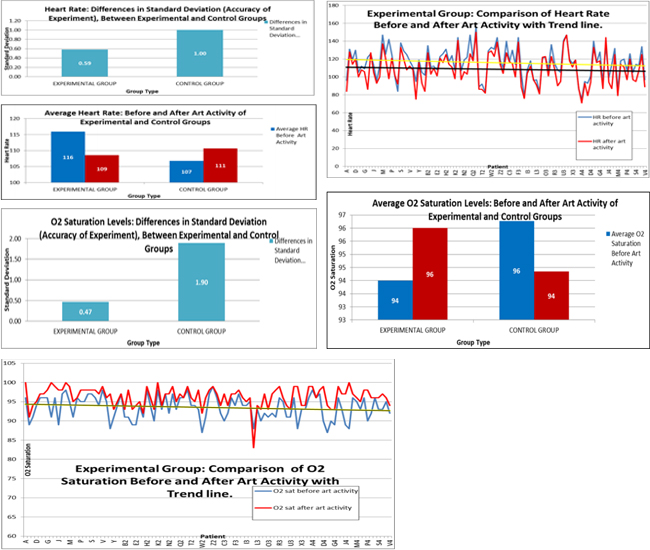
CONCLUSION
This study clearly indicated a physiologic relaxation response to the art activity. Stress levels were measured by the biomarkers of heart rate and oxygen saturation. There was a consistent decrease in the heart rate and an increase in the oxygen saturation level during and after the art activity. Most of the children were not in pain at the time of the activity, therefore, minimal data was obtained on changing pain levels. Affect and demeanor improved in almost all of the children. Patients, families, and staff all seemed to appreciate the art activities. Parents would often use the time the art facilitator spent with the child to take a break from caregiving and frequently expressed gratitude for this service. It is important to investigate the use of non-pharmacological techniques to help children cope with stressful hospital experiences. Giving these children an opportunity to express themselves through art clearly has a therapeutic effect physiologically and can become part of the healing process.
REFERENCES
- Councill T. (2003). Medical art therapy with children. In Malchiodi, C. A. (Ed), Handbook of art therapy. New York: Guillford Publications. (Ed), Medical art therapy with children. London: Jessica Kingsley Publishers.
- DeLue CH. (1999). Physiological effects of creating mandalas.
- In Malchiodi C, Dionigi A and Gremigni P. (2016). A combined intervention of art therapy and clown visits to reduce preoperative anxiety in children. Journal of Clinical Nursing, 26: 632-640.
- Koller D. (2008). Child Life Council Evidence-Based Practice Statement. Therapeutic Play in Pediatric Health Care: The Essence of Child Life Practice.
- Malchiodi CA. (1993). Introduction to special issue: Art and medicine. Art Therapy: Journal of the American Art Therapy Association, 10(2): 66-69.
- Malchiodi CA. (Ed). (1998). The art therapy sourcebook. Lincolnwood, IL: Lowell House.
- Malchiodi CA. (Ed). (1999). Medical art therapy with children. London: Jessica Kingsley Publishers.
- Madden J, Mowry P, Gao D and Cullen P. (2010). Creative Arts Therapy Improves Quality of Life for Pediatric Brain Tumor Patients Receiving Outpatient Chemotherapy. Journal of Pediatric Oncology Nursing, 27(3): 133-145.
- Palmer J and Nash F. (1991). The hospital arts movement. International Journal of Arts Medicine, 1(1): 34-39.
- Prager A. (1993). The art therapist's role in working with hospitalized children. American Journal of Art Therapy, 32(1): 2.
- Rode D. (1995). Building bridges within the culture of pediatric medicine: the interface of art therapy and child life programming. Art Therapy: Journal of the American Art Therapy Association, 12(2): 104-110.
- Rollins J, Drescher J and Kelleher M. (2012). Exploring the ability of a drawing by proxy intervention to improve the quality of life for hospitalized children. Arts and Health. 4(1): 55-69.
- Siegel BS. (1990). Love, medicine and miracles. New York: Harper and Row.
- Sundaram R. (1995). In focus: Art therapy with a hospitalized child. American Journal of Art Therapy. 34(1): 2-8.
- Sznewajs P. (2009). To the next power: How true cultural partnerships can exponentially grow a hospital arts program. Arts and Health. 1(2): 183-189.
- Wallace J, Packman W, Huffman L, Horn B, et al. (2014). Psychosocial changes associated with participation in art therapy interventions for siblings of pediatric hematopoietic stem cell transplant patients. Art Therapy: Journal of the American Art Therapy Association, 31(1): 4-11.
- Wikstrom, B-M. (2005). Communicating via expressive arts: The natural medium of self-expression for hospitalized children. Pediatric Nursing. 31(6): 480-485.
- Yount G, Rachlin K and Siegel J. (2013). Expressive arts therapy for hospitalized children: a pilot study measuring cortisol levels. Pediatric Reports. 5(e7): 28-30.