Previous Issues Volume 1, Issue 4 - 2016
Double Pylorus: A Report of Two Cases
Lei Shi1, Fu-Jian Liu1
1Department of Gastroenterology, Eighth Affiliated Hospital of Guangxi Medical University, Guigang 537100, Guangxi Zhuang Autonomous Region, China.
Corresponding Author: Lei Shi, Department of Gastroenterology, Eighth Affiliated Hospital of Guangxi Medical University, Guigang 537100, Guangxi Zhuang Autonomous Region, China, Tel: +86 775 4200028; E-Mail: [email protected]
Received Date: 27 Sep 2016 Accepted Date: 15 Oct 2016 Published Date: 20 Oct 2016
Copyright © 2016 Shi L
Citation: Lei Shi and Fu-Jian L. (2016). Double Pylorus: A Report of Two Cases. Mathews J Case Rep 1(4): 016.
ABSTRACT
Double pylorus is one of the rarest anomalies of the stomach and has been reported in 0.001-0.4% of upper gastrointestinal endoscopies. Congenital abnormalities are very rarely found during gastrointestinal endoscopy in adults. We present 2 typical cases of double pylorus, including a case of congenital double pylorus in a 64-year-old man. We describe the clinical features, physical examination, and endoscopic findings of these cases.
KEYWORDS
Double Pylorus; Peptic Ulcer; Abdominal Pain; Anti-Ulcer Medication.
INTRODUCTION
Double pylorus, also known as duplication of the pylorus, is one of the rarest anomalies of the stomach, consisting of 2 openings connecting the antrum to the duodenal bulb [1]. A review of the literature found approximately 100 published cases since 1969. It can be congenital or acquired. Acquired double pylorus is more commonly observed, and is a complication of peptic ulcer resulting from intramural penetration by the ulcer [2]. Here, we report 2 typical cases from China, including a case of congenital double pylorus.
CASE PRESENTATION
The first patient was a 64-year-old man who was referred to our department with approximately 2 months of epigastric discomfort. Upper gastrointestinal endoscopy revealed 2 communicating channels between the gastric antrum and the first part of the duodenum (Figure 1). No signs of peptic ulcer or scarring were noted. Histological examination of both channels showed mild gastritis (Figure 2). Therefore, the case was considered to be congenital in origin. The second patient was a 67-year-old man admitted on an emergency basis because of abdominal pain, with 10 days of abdominal distention. Endoscopy identified a double pylorus deformity; the second duct was acquired and originated from an ulcer located in the duodenal bulb, with penetration of the prepyloric antrum (Figure 3). Biopsies of the ulcerative region showed active atrophic chronic gastritis (Figure 4). Testing for Helicobacter pylori was negative. An acquired double pylorus was diagnosed. Gastroscopy 4 weeks later revealed resolution of the inflammatory changes with ulcer reepithelization, but the double pylorus remained (Figure 5). Biopsy of the gastric mucosa again showed atrophic chronic gastritis (Figure 6). In both cases, no abnormal findings were revealed on physical examination and laboratory testing. The patients were successfully treated conservatively with anti-ulcer medication. We recommend use of anti-ulcer medication as the treatment of choice for double pylorus.
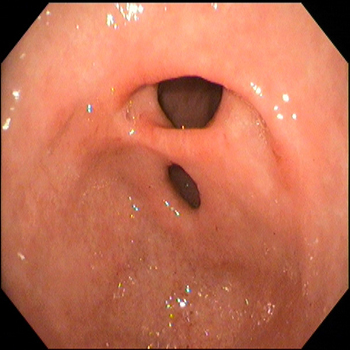
Figure 1: Upper gastrointestinal endoscopy revealed 2 communicating channels between the gastric antrum and first part of the duodenum.
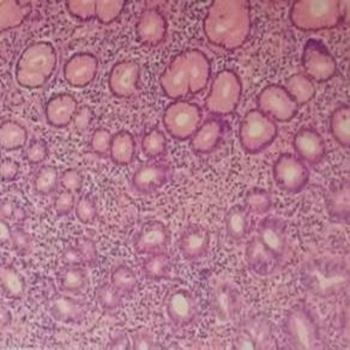
Figure 2: Histological examination showed mild gastritis (x400).
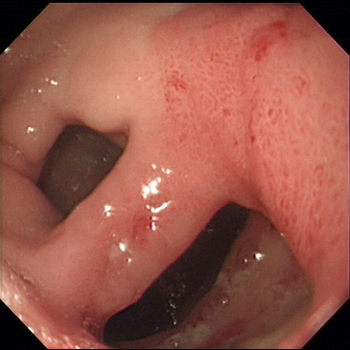
Figure 3: Endoscopic findings identified a double pylorus deformity; the second duct was acquired and originated from an ulcer located in the duodenal bulb, with penetration of the prepyloric antrum.
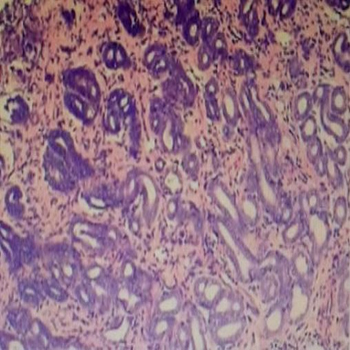
Figure 4: Biopsies of the ulcerative region showed active atrophic chronic gastritis (x400).
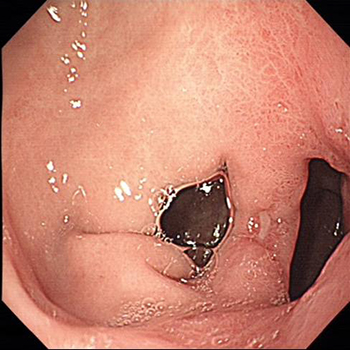
Figure 5: Gastroscopy at 4 weeks revealed resolution of the inflammatory changes with ulcer reepithelization, but the double pylorus remained.
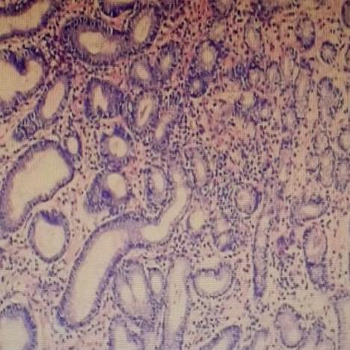
Figure 6: Repeat biopsy of gastric mucosa revealed atrophic chronic gastritis (x400).
DISCUSSION
Double pylorus is usually defined as an abnormal pylorus located near the normal pylorus, and is an extremely rare anomaly of the intestinal tract. The first reported case was published in 1969 by Smith, who described a patient with a double pylorus [3]. Double pylorus can occur as either a congenital abnormality or an acquired complication of peptic ulcer disease. Most reported cases of double pylorus have been associated with the presence of chronic peptic ulcers, thus indicating an acquired origin of the condition. Congenital duplications of the pyloric channel are very rare [4]. The specific causes and development of a double pylorus are unknown. A congenital double pylorus seems to develop from a localized abnormality of the lateral pylorus process at an early embryonic stage [5]. Acquired double pylorus results from peptic ulcer erosion, with development of a fistula between the duodenal bulb and distal stomach. Ingestion of nonsteroidal anti-inflammatory drugs contributes to persistence of peptic ulcer disease [6]. In this study, we present 2 typical cases of double pylorus, including a case of congenital double pylorus in a 64-year-old man. We describe the clinical features, physical examination, and endoscopic findings of these cases. The diagnosis was based on the results of gastrointestinal endoscopy and histological features of the 2 channels. Although the causes and development of this rare entity remain speculative, conservative treatment with antacids is advocated by the literature [7]. In most studies, the patients responded well to conservative treatment for peptic ulcers, regardless of whether the fistula remained open or spontaneously closed [8]. In general, this abnormality tends to be clinically silent, and is mostly found incidentally by endoscopy performed for other indications [9, 10]. Surgical intervention is required only for refractory symptoms, recurrent ulcers, and other complications [11]. Treatment with anti-ulcer medication must be promptly instituted and biopsies from the ulcer and pseudopylorus are essential to exclude gastric adenocarcinoma [12].
REFERENCES
- Mylonas A, Papaziogas B, Paraskevas G, Fragos E, et al. (2002). Congenital double pyloric ostium in the adult. Surg Endosc. 16(11), 1639.
- Hu TH, Tsai TL, Hsu CC, Lu SN, et al. (2001). Changchien CS. Clinical characteristics of double pylorus. Gastrointest Endosc. 54(4), 464-470.
- Smith VM and Tuttle KW. (1969). Gastroduodenal (pyloric) band. Endoscopic findings and first reported case. Gastroenterology. 56(2), 331-336.
- Kothandaraman KR , Kutty KP, Hawken KA and Barrowman JA. (1983). Double pylorus--in evolution. J Clin Gastroenterol. 5(4), 335-338.
- Berrocal T, Torres I, Gutierrez J, Prieto C, et al. (1999). Congenital anomalies of the upper gastrointestinal tract. Radiographics. 19(4), 855-872.
- Wallace JL. (2000). How do NSAIDs cause ulcer disease? Baillieres Best Pract Res Clin Gastroenterol. 14(1), 147-159.
- Wolters VM, Nikkels PG, Van Der Zee DC, Kramer PP, et al. (2001). A gastric diverticulum containing pancreatic tissue and presenting as congenital double pylorus: case report and review of the literature. J Pediatr Gastroenterol Nutr. 33(1), 89-91.
- Hu TH, Tai DI, Changchien CS, Chen TY, et al. (1995). Double pylorus: report of a longitudinal follow-up in two refractory cases with underlying diseases. Am J Gastroenterol. 90(5), 815-818.
- Arhan M, Oztas E, Ibis M, Sezgin S, et al. (2010). A rare endoscopic finding: acquired double pylorus.Surg Endosc. 24(1), 244-245.
- Akazawa Y, Mizuta Y, Osabe M, Nakamura T, et al. (2005). A case of double pylorus caused by recurrent gastric ulcers: a long-term endoscopic observation. Dig Dis Sci. 50(11), 2125-2128.
- Yoshimura Y, Yasutake K, Imamura Y and Oimomi M. (1988). Double pylorus accompanied by gastric ulcer resistant to H2-receptor antagonist--a case report and review of the literature. Kobe J. Med Sci. 34(4), 151-159.
- Fine M, Kavin H and Grant T. (1987). Double-channel pylorus as a complication of carcinoma of the stomach. Gastrointest Endosc. 33(1), 39-41.