Previous Issues Volume 1, Issue 1 - 2016
Comorbid Depression in Association with Generalized Anxiety Disorder and Panic Disorder, in a Young Patient with Facet Joints Spondylosis of the Lumbar Spine
Ahmed Al-Imam1,2,3
1Doctoral Student (PhD in Medicine), School of Life and Medical Sciences, University of Hertfordshire Doctoral College, Hertfordshire University, AL10 9AB, Hatfield, Hertfordshire, United Kingdom.
2Lecturer and Researcher at the Department of Anatomy and Cellular Biology, College of Medicine, University of Baghdad, Bab Al-Mo'adham, 10047, Baghdad, Iraq.
3Member of National Academy of Neuropsychology (NAN). Member of European Academy of Dermatology and Venereology (EADV). Member of American Association of Anatomists (AAA).
Corresponding Author: Ahmed Al-Imam, Doctoral Student (PhD in Medicine), School of Life and Medical Sciences, University of Hertfordshire Doctoral College, Hertfordshire University, AL10 9AB, Hatfield, Hertfordshire, United Kingdom. Tel: +964 (0) 771 433 8199; E-Mail: [email protected] Received Date: 18 Apr 2016 Accepted Date: 02 May 2016 Published Date: 09 May 2016 Copyright © 2016 Al-Imam A. Citation: Al-Imam A. (2016). Comorbid Depression in Association with Generalized Anxiety Disorder and Panic Disorder, in a Young Patient with Facet Joints Spondylosis of the Lumbar Spine. Mathews J Psychiatry Ment Health. 1(1): 002.
ABSTRACT
This is a challenging case of a young 32-years old male patient. His psychiatric-medical condition lasted for around three years, from late 2012 to late 2015. Almost all of the patient's problem in this case scenario, originated from an imbalanced relationship with an older female colleague with a wider experience of life, including sexual life. This relation was a source of psychological disturbances that gradually became interfering with patient's routine daily life, work and professionalism, social life, family relationships, and his overall progress as a functioning individual in his society. Patient psychological distress, arose from a depriving relationship with his female colleague. His distress, was centered about the female's past sexual life, including her past marital life, and her pre-marital experience with multiple sexual partners. The patient became gradually convinced that the female was in desperate need of his persistent support to overcome her recent divorce issue, which eventually depleted the patient at emotional, psychological, and physical levels. Later, the patient developed a parallel medical condition, which is facet joints' degeneration (osteoarthritis) of the lumbar spine, in the context of mild-to-moderate lower lumbar spondylosis that was most evident at L4-L5 and L5-S1 intervertebral levels. His persistent lumbar back pain, became a two-faceted player, interfering with patient's daily physically activity, and causing significant emotional distress, depression, anxiety, and even panic attacks sporadically. This physical illness added to the already burdened psychological status. His lumbar spine problem persisted for approximately an entire year that was eventually dramatically improved in late 2015. After which, the patient gradually resumed his daily activities, including working as professional member of the teaching staff at a University level. There were no residual effects interfering with psychological improvement, apart from sporadic and negligible flash backs of his emotionally-traumatic experience. However, these were insignificant, and never interfering anymore with his normal life and interpersonal communications. In summary, this case provides a further embodied evidence, of how a psychologically-related disturbance, at an emotional level, can be of potential physical consequences, and vice versa. Moreover, the physical illness of this patient, played key role in augmenting, impending, and delaying the full psychological recovery.
KEYWORDS
Case report; Depression; Anxiety; Young; Lumbar; Facet joints; Zygapophyseal; Degeneration; Spondylosis; Physiotherapy.
INTRODUCTION
Generalized anxiety disorder (GAD) is a common psychiatric condition, and it is usually more common in females. The associated individual and societal burden, is substantial. GAD is characterized by excessive and inappropriate worrying that is persistent for months, and not restricted to particular circumstances, in which patients develop somatic symptoms (such as palpitations, tremors, dyspnea, and others) and psychologic (psychic) symptoms. Epidemiological studies from Europe, suggests that GAD lifetime prevalence is around 4.3-5.9%. Patients with comorbid major depression and GAD, tend to have a more severe and prolonged course of illness with greater functional impairment. GAD represents a multifactorial developmental disorder of a genetic-environmental interaction that culminates in structural and functional changes in the amygdala-prefrontal circuitry. Many psychotropic drugs are available for the treatment of patients with GAD. Substantial evidence in literature, support the efficacy of certain Selective serotonin reuptake inhibitors (SSRIs), Serotonin and norepinephrine reuptake inhibitors (SNRIs), pregabalin and quetiapine. However, the ideal treatment for GAD, should be determined by the clinical features of the patients, presence of comorbidities including depression, patient's preferences for drugs, and therapeutics' availability [1]. Psychotherapy, behavioral modification therapy, and cognitive therapy also play vital role in managing GAD. Cognitive therapy, whether alone or combined with medications, provides a viable option in the treatment of outpatients with primary, non-bipolar depression. Additionally, cognitive therapy alone seems to be an effective alternative to tri-cyclic antidepressants [2].
Panic disorder (PD) is a chronic and disabling condition that is often accompanied by other psychiatric and medical conditions, including GAD. The lifetime prevalence of PD, is approximately 4.7%. The SSRIs and SNRIs, are also used to effectively manage PD, as in GAD. Escitalopram is proved to be a highly selective SSRI, and the available evidence points to it, as of great value in the treatment of PD. Further, patients with PD, are at an increased risk for suicide, which seems to be greater in patients with a comorbid depression. Escitalopram has the potential to reduce numerous related symptoms. Additionally, compared to Tricyclic Antidepressants (TCAs) and Monoamine oxidase inhibitors (MAOIs), it has a favorable tolerability that predicts a more successful initiation and maintenance, and a safer risk profile [3]. However, TCAs appears to have an additional analgesic property when compared to escitalopram, by acting to reduce the sensory discriminative component via potentiating pain modulatory systems. Therefore, TCAs can be used in GAD/PD patients that already have painful comor bidities [4]. In this case report, TCAs is also used for its analgesic effect in a patient with lumbar spine problem (facet joints' spondylosis), which is a localized form of osteoarthritis (OA) of the spine, that involves the facet joints (zygapophyseal joints). Facet joint osteoarthritis (FJOA) is intimately linked to the distinct but functionally related condition of degenerative intervertebral disc disease, and both have an enormous impact on the health-care systems and economies of developed countries. FJOA is defined as a functional failure of the synovial facet joints, due to variable degrees of damage/loss to the articular synovial cartilage. Radiographic hallmarks of FJOA, include narrowing of the facet joint space, subarticular bone erosions, subchondral cysts, osteophyte formation, and hypertrophy of the articular process. Cross-sectional imaging with CT or MRI is required for a detailed evaluation of facet joint morphology. Amongst community-based adults in the Framingham Heart Study, moderate or severe lumbar FJOA on CT imaging was present in 36% of adults of age below 45 years, and the prevalence was found to be incremental with older age groups. Risk factors for FJOA include age, sex, overweight, physical trauma, occupational factors, smoking, and others. Alterations in the structural integrity of the three-joint complex (two facet joints and one intervertebral), particularly the intervertebral joint degeneration (IJD) of the same vertebral segment(s), as well as abnormal joint alignment or loading and paraspinal muscular weakness are implicated as risk factors for development of FJOA [5]. In FJOA, facetogenic spinal pain, is a frequent and a debilitating cause of mechanical spine pain. Diagnostic blocks, including medial branch blocks (MBBs) are the only reliable approach to identify facet joints as the source of spinal pain. In the absence of a reference standard, MBBs actually serve more of a prognostic than diagnostic role, enabling the selection of patients who might respond to radiofrequency denervation treatment, which is the standard treatment for facet joint pain. On contrary, trials of intra-articular steroid injections including Depo-Medrone injections, for lumbar and cervical facet joint pain, have yielded disappointing results and also lasting for no more than three months, while, radiofrequency denervation provides some benefit for up to a year in approximately 60% of individuals [6]. Clinical and radiological data, revealed that FJOA and IJD, appear to coexist and augment each other pathology in a reciprocal manner leading to spinal pain. However, how these latter two conditions are related to each other in terms of their development, is not fully understood [7].
CASE REPORT
The patient, Mr. N.T., is a 32 years old male from Baghdad, Iraq. He was completely healthy and athletic, apart from an asymptomatic hemangioma in the right lobe of the liver, approximately nine millimeters in diameter, that was diagnosed accidently during an abdominal ultrasonography in august 2014. In late 2012, the patient became involved in a confusing emotional relationship, with an older female colleague, while they were studying the same post-graduate course via distance-learning. The female was older by eight years than the patient. She was already divorced, with three children, and she was from a different religious, ethnic, cultural backgrounds, and she lived in a distant country on an entirely different continent. The female had prior martial and pre-marital emotional relationships, and she kept involving her male colleague (the patient), with details about these relationships, that goes back as far as the age of 15 years old. After a relatively short period of time, around three to four months, the patient started to gradually develop neurotic signs and symptoms, that manifested as disturbances with patient's social life, his work, and relationship with key family members including his parents. Similarly, He became gradually withdrawn from social life, and more focused on his female colleague, who became the absolute center of his attention. Approximately, two years later, they met together abroad. Their meeting was justified by studying again together at a post-graduate institution (a university in Europe), where they became gradually more emotionally involved for about four months. In January 2015, the patient suffered from an acute back injury, due to lifting his female colleague on few occasions. He consulted the university's medical counselling services, for several times for his persistent localized lumbar back pain, and he was wrongly diagnosed by general practitioners (GP) on three different occasions, with a torn erector spinae muscle. He was prescribed with pain killers, mainly Naproxen 500 mg tablets on need, and Diazepam 5 mg tablets at night. Additionally, the GPs insisted on the patient to remain mobile, active, and engage in normal daily activities. Three weeks later, his pain became more persistent, frequent and more complicated by occasional sports activities, including Basketball and football. He re-consulted his GP at the university, who kept insisting that his condition is merely due to a torn paraspinal extensor muscle. The patient later became very involved with his studies and exams, and kept using analgesia for symptomatic relief of his frequent back pain. In parallel to his medical condition, the patient also consulted the university's mental counselling services, concerning his persistent obsessions and anxiety, concerning the females past sexual life. During one of the counselling sessions, the patient was advised against this harmful relationship and to "be protected from a depriving relationship". However, the patient ignored this opinion. On March 2015, the patient had a very harsh verbal argument in public with his female colleague concerning her past sexual life, and their relationship ended completely at that point. At this point of time, the patient was suffering from his yet undiagnosed lumbar spine injury, and his emotional mental storm (break-up). Within few days, he did a medical consultation for his back problem at a specialist rheumatologist clinic. The rheumatologist immediately asked for radiological analysis of his case, specifically Magnetic Resonance Imaging (MRI) of his thoracic and lumbosacral spine, and pelvis. The MRI report and the specialist opinion, were congruent to confirm the diagnosis of mild-to-moderate spinal spondylosis of the lumbar spine, which evidently worst at the level of L4-L5 and L5-S1 (figure 1), at which there was facet joints' degeneration and an accompanying mild circumferential bulge of the intervertebral disc bulge into the adjacent spinal canal, with minimal intervertebral disc degeneration at L5-S1. Luckily, there was no definite neural impingement. The main focus of pain was the right facet joint at L5-S1, where the rheumatologist decided to infiltrate the affected joint with Depo-Medrone and a local anesthetic, the procedure was done under fluoroscopy guide. The patient was also prescribed Etoricoxib 90mg tablet once a day for 10 days, and diazepam 5 mg tablet once daily for a week.
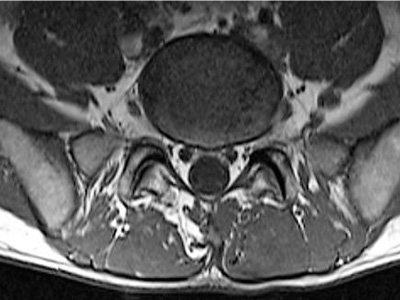
Figure 1:A cross sectional MRI of the lumbar spine, showing facet joint degeneration at the level of L5-S1, with a mild circumferential disc bulge. Similar findings were also found at L4-L5 level.
The physician high recommended the patient to undergo physiotherapy as soon as possible to strengthen his paraspinal and abdominal muscles. Within a week, the patient travelled to meet his family for social support, and he also underwent 20 sessions of physiotherapy. Physiotherapy included transcutaneous electrical nerve stimulation (TEN), muscle stretching techniques, heat therapy, passive and active exercises, and Low-level laser therapy (LLLT) for his lumbar spine. Simultaneously, the patient sought a psychiatrist consultation, the psychiatric evaluation was in line with the medical report provided by the university's mental counselling specialists. Quoted from the University psychiatric evaluation, this statement "the relationship has ended but he (the patient) is still feeling anxious and preoccupied, this is affecting his day-to-day living". Both professional psychiatrists' evaluation, was congruent to diagnose the patient with a GAD and depression. The psychiatrist prescribed amitriptyline 25 mg tablets once daily at night, and Escitalopram 10 mg tablets over a week, once daily at morning. The patient was compliant with all his medication, with exception of Escitalopram, because the tablets were not available at the local pharmacies at that moment. Moreover, the patient was forced to travel back to his university on April 2015, to solve his interim suspension decision that was issued by the university against him, the suspension decision was based upon a complaint filed by his female colleague at the day of their public verbal argument. The suspension decision was later removed, and the patient got back to his country on June 2015, where he kept suffering of periodic lumbar backache (lumbago) that further augmented his depressive mood patterns, he also developed few panic attacks mainly at night. The psychiatrist consultation, insisted to initiate management with Escitalopram 10 mg tablets, to control his panic disorder (PD). Within one month of being compliant with his medications, and using the family support that he had available and particularly from his mother, his panic attacks disappeared and his depressive started to regress. The patient was compliant to all his prescribed medications, physiotherapy, and persisted on swimming to improve his back strength, particularly the paraspinal muscles. He kept taking oral analgesic medications, in the form of Loxoprofen Sodium 60 mg tablets three times daily, and Eperisone 50 mg tablets three times a day, both were eventually tapered over a month to one tablet a day, and was later discontinued. He also took daily tablets of nutritional supplements containing multivitamins, minerals, chondroitin sulfate, and glucosamine for six months' period, these supplements were recommended by a professional pharmacist, and the patient subjectively reported them to be effective in improving his condition. He started to gain some of his routine daily activity by September 2015, his pain was less, and his psychiatric status was fine apart from sporadic depressive episodes, while panic attacks were completely absent. As mentioned earlier, his medications for depression and panic attacks, were gradually tapered, then completely discontinued. He resumed working as a professional member of the teaching staff on February 2016. He was able to engage well in social life, with normal interpersonal relations. However, there were some flash back memories in relation to his past traumatic emotional experience, that were sporadic, but they are no longer interfering to any degree, with neither mood status nor patient's normal life.
DISCUSSION AND CONCLUSION
This case represents a provocative case that required patience and persistent follow-up of the patient. The complications arose from the co-existence of chronic psychiatric problem, and a chronic lumbar back pain as a result of facet joints' spondylosis of the lumbar spine. The back pain was often very distressing, and highly interfering with daily physical activities for almost an entire year, stating from January in 2015, to the point that the patient thought that he will be disabled by his condition indefinitely. Family support, particularly maternal, was a corner stone for patient's recovery, and it was paralleled by therapeutic intervention from a specialist rheumatologist, a psychiatrist, and physiotherapist. All worked within the context of an inter- and multi-disciplinary team (MDT) approach. Physiotherapy and swimming, were highly successful adjuncts to the therapeutic intervention including cognitive psychotherapy, all were vital for successful resolution of this two-faceted intriguing case of a young man. In October 2015, the patient was scheduled for a medial branch blocks (MBBs) procedure and a subsequent radiofrequency ablation, under fluoroscopy guide, to abolish the afferent neural pain pathway originating at the level of the affected/ degenerative facet joint(s). However, this procedure was later cancelled due to patient improvement. In late 2015, the patient started to recover substantially at all levels, including psychologically, and he is currently resuming his life normally, apart from insignificant sporadic flash backs, that are never interfering with his daily routine or interpersonal relationships. In conclusion, this case embodies, the true meaning physicalpsychological interaction of an illness in a young male patient. Both hindered the medical intervention of the other, and led to a delay of a full recovery, that lasted approximately for an entire year from January 2015 to late 2016. While the psychological roots of this problem, date back to late 2012, from a depriving relationship with an older female colleague.
REFERENCES
- Baldwin DS, Waldman S and Allgulander C. (2011). Evidence- based pharmacological treatment of generalized anxiety disorder. The International Journal of Neuropsychopharmacology, 14(05), 697-710.
- Beck AT, Hollon SD, Young JE, Bedrosian RC, et al. (1985). Treatment of depression with cognitive therapy and amitriptyline. Archives of general psychiatry. 42(2), 142-148.
- Townsend MH and Conrad EJ. (2007). The therapeutic potential of escitalopram in the treatment of panic disorder. Neuropsychiatric disease and treatment. 3(6), 835-838.
- Sharav Y, Singer E, Schmidt E, Dionne RA, et al. (1987). The analgesic effect of amitriptyline on chronic facial pain. 31(2), 199-209.
- Gellhorn AC, Katz JN and Suri P. (2013). Osteoarthritis of the spine: the facet joints. Nature Reviews Rheumatology. 9(4), 216-224.
- Cohen SP, Huang JH and Brummett C. (2013). Facet joint pain-advances in patient selection and treatment. Nature Reviews Rheumatology. 9(2), 101-116.
- Li J, Muehleman C, Abe Y and Masuda K. (2011). Prevalence of facet joint degeneration in association with intervertebral joint degeneration in a sample of organ donors. Journal of Orthopaedic Research. 2011 29(8), 1267-1274.