Previous Issues Volume 2, Issue 1 - 2017
Burden of Atrial Fibrillation in Patients with Spontaneous Intracerebral Hemorrhage in Florence District over the Years
Luca Masot1, 2*, Federico Moroni1, Vieri Vannucchi1, Elisa Grifoni2, Giancarlo Landini1, Filippo Cellai3, Stefano Spolveri4, Mauro Pratesi5, Anna Poggesi6, Domenico Inzitari6
1Department of Internal Medicine, Santa Maria Nuova Hospital, Florence, Italy.
2Department of Internal Medicine, San Giuseppe Hospital, Empoli, Italy.
3Department of Informatic and Health Technologies, ESTAR, Tuscany, Italy.
4Department of Internal Medicine, Borgo San Lorenzo Hospital, Florence, Italy.
5Department of Emergency, Santa Maria Nuova Hospital, Florence, Italy.
6Neuroscience Section, Department of Neurofarba, University of Florence, Florence, Italy.
Corresponding Author: Luca Masotti, Internal Medicine, Santa Maria Nuova Hospital, Piazza Santa Maria Nuova 1, 50122 Florence, Italy, Tel: 00855-16-241-666; E-Mail: [email protected]
Received Date: 22 Mar 2017 Accepted Date: 22 May 2017 Published Date: 26 May 2017 Copyright © 2017 Masotti L Citation: Bhalla D and Lotfalinezhad E. (2016). A Short Perspective on the Risk Profile of Epilepsy in Iran. Mathews J Neurol. 1(1): 003.
ABSTRACT
Background and aim: Literature evidence about the burden of atrial fibrillation (AF) in patients with spontaneous intracerebral hemorrhage (ICH) is lacking. Therefore, the aim of our study was to answer this issue.
Materials and methods: We reviewed the International Classification of Diseases, 9th revision, Clinical Modification (ICD- 9th CM) database referred to patients discharged from the six Hospitals of Florence district, Italy, in a 15-year period (2001- 2015). Code 431 (spontaneous ICH) was searched as primary or secondary diagnosis, and then matched with code 427.31 (AF) in one of the other discharge diagnoses.
Results: Overall, 7452 patients were discharged with ICH as primary or secondary diagnosis. Of them, 693 (9.2%) had AF. The burden of AF increased with age (1.5% in patients under the age of 65 years, 6.4% in patients aged 65-75 years, and 12.8% in those older than 75 years), and over the years (5.6% in 2001, 8.9% in 2008, and 11.4% in 2015), irrespective of age. In-hospital mortality decreased over the years both in patients with and without AF. However, in-hospital mortality in patients with AF-related ICH was significantly higher than in patients without AF (29.4% vs 23.3%, p=0.04).
Conclusion: Our study demonstrates that, in patients with spontaneous ICH, the burden of AF is absolutely not negligible, and seems to be increasing over the years.
KEYWORDS
Intracerebral Hemorrhage; Atrial Fibrillation; Burden; Mortality.
INTRODUCTION
Atrial fibrillation (AF) is the most commonly found arrhythmia in clinical practice, and represents a public healthcare problem worldwide. Its incidence and prevalence increase steadily with age. Prevention of AF-related cardio embolism, and especially of embolic strokes, which represent about one third of all ischemic strokes, is one of the main goals of AF treatment [1]. Oral anticoagulation, both with direct oral anticoagulants (DOACs) and vitamin K antagonists (VKAs), represents the treatment of choice for preventing cardio embolism [1]. Therefore, in the last decades many efforts have been made to increase physician's confidence in the appropriate management of AF.
Due to high acute mortality and severe neurological disability, spontaneous intracerebral hemorrhage (ICH) represents the most devastating stroke subtype [2]. The 30-day mortality rate approaches 40%, and seems to have remained unchanged over the last 30 years [2]. In the acute phase, few specific treatments, such anti-hypertensive drugs and reversal therapy in coagulopathy-associated ICH, are available only for selected patients, and their benefits are questionable. Literature evidence about the real burden of AF in patients with spontaneous ICH is lacking. Therefore, the aim of our study was to provide answer to this issue.
MATERIALS AND METHODS
We reviewed the International Classification of Diseases, 9th revision, Clinical Modification (ICD-9th CM) database referred to patients discharged from the six Hospitals of Florence district (Careggi Hospital, Santa Maria Nuova Hospital, Santa Maria Annunziata Hospital, San Giovanni di Dio Hospital, Figline Valdarno Hospital and Borgo San Lorenzo Hospital), Tuscany, Italy in a 15-year period (2001-2015). Code 431 (spontaneous ICH) was searched as primary or secondary diagnosis, and then matched with code 427.31 (AF) in one of the other discharge diagnoses. The endpoints of this research were the number of cases of spontaneous ICH and AF, and the number of deaths occurred every year in patients with spontaneous ICH associated or not with AF. The burden of AF in patients with spontaneous ICH, and in-hospital mortality were reported as percentage of diagnoses.
RESULTS
Overall, 7452 patients were discharged with ICH as primary or secondary diagnosis. Of them, 3695 (49.5%) were females. 4363 patients (59.1%) were 75-years old and older, whereas 1678 (22.5%) were 65-75 years old, and 1411 (18.4%) under the age of 65 years. Six hundred and ninety-three patients (9.2%) had AF. The burden of AF increased with age (1.5% in patients under the age of 65 years, 6.4% in patients aged 65- 75 years, and 12.8% in those older than 75 years), and over the years (5.6% in 2001, 8.9% in 2008, and 11.4% in 2015) (Figure 1), irrespective of age. In-hospital mortality decreased over the years both in patients with and without AF (Figure 2). However, in patients with AF-related ICH, in-hospital mortality was significantly higher than in those without AF (29.4% vs 23.3%, p=0.04).
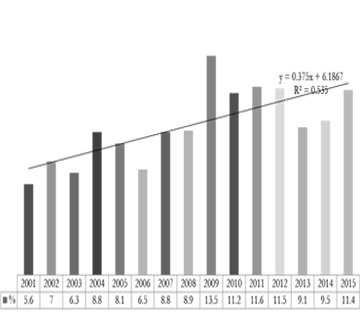
Figure 1: Trend in the burden of atrial fibrillation in patients with spontaneous ICH.
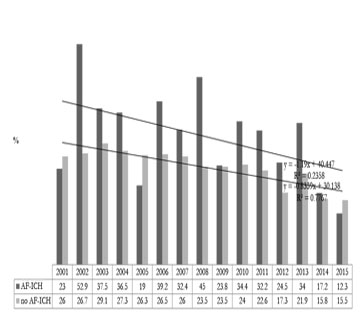
Figure 2: Trend in in-hospital mortality in atrial fibrillation-related spontaneous ICH.
DISCUSSION
The real burden of AF in patients with spontaneous ICH is unknown. McGrath ER et al. found that, in patients with AF, no risk factor has a strong association with ICH, except for VKAs oral anticoagulants intake, especially if International Normalized Ratio (INR) is higher than 2.0 [3]. Horstmann S et al. found that, 90 days after spontaneous ICH, AF was diagnosed in 64 of 206 patients (31.1%). The 3-month mortality was significantly higher in patients with AF than in those without (45.3% vs 31%) at univariate analysis; however, after adjustment for co-morbidity and oral anticoagulant treatment, AF did not remain an independent predictor of mortality [4]. In a study performed in two Italian Hospitals on 470 consecutive patients with spontaneous ICH, AF was associated with a 3-fold increased risk of poor outcome (OR 3.18, 95% CI, 1.12-9.05, p=0.03) [5].
Our study focused on hospital discharge diagnoses along a 15-year period in a metropolitan Italian town encompassing about one million inhabitants. We demonstrated that, in patients with spontaneous ICH, the burden of AF is absolutely not negligible, and seems to be increasing over the years. Indeed, up to now, more than one of ten patients had concomitant AF. The burden of AF in spontaneous ICH seems to have doubled over the years, increasing from 5.6% in 2001 to 11.4% in 2015. To the best of our knowledge, this is the first literature report focusing on the trends of AF in spontaneous ICH. The reason of our finding is unclear. The incidence and prevalence of AF increase steadily with age. In the United States, the incidence of AF in the general population aged 80 years and older is around 9%, whereas in Europe 17.8% of people aged 85 years and older has AF [6-8]. In our study, 81.6% of patients discharged with diagnosis of spontaneous ICH were 65-years old and older. Therefore, our data could reflect the epidemiological burden of AF in the general population. Moreover, oral anticoagulants or antiplatelets may have played a role as favoring factors for ICH in our population. Despite oral anticoagulation, especially with VKAs, is still underused, in the last few years its prescription has been increasing, and literature evidence shows a parallel increase in the burden of oral anticoagulant-related ICH [9-13]. Moreover, it is important to remark that many patients suffering from AF receive antiplatelets for cardio embolism prevention, and that antiplatelets, represent up to now the class of antithrombotic drugs most frequently associated with non-traumatic ICH [14].
Despite prognosis of spontaneous ICH seems to have remained unchanged over the years, steps forward have been made in the latest years, such as a better prognostic stratification by using clinical practice grading scales or neuro-radiological findings (i.e. spot sign), a wider use of reversal strategies in coagulopathy-related ICH, a better anti-hypertensive treatment, the allocation of patients in appropriate settings (stroke units or neurointensive care), and, finally, a better global approach to complications, such as dysphagia, infections or venous thromboembolism. In our study, in-hospital mortality in patients with spontaneous ICH, both associated or not with AF, decreased over the years. The reduced mortality could be secondary to a better global approach in the acute phase of ICH. In patients with spontaneous AF-related ICH taking oral anticoagulants, the reduced mortality could be ascribed to the wider use of reversal strategies. In-hospital mortality in patients with AF-related ICH was significantly higher than in those without AF. This higher in-hospital mortality in AF patients could be due to more severe bleeding and/or more frequent hematoma enlargement and neurological deterioration in patients taking anticoagulants or antiplatelets for cardio embolism prevention [15].
We recognize that our study has many limitations, mainly due to its retrospective design. Diagnosis coding by using the ICD- 9th CM is operator dependent; therefore, coding bias could have been included in our study. Moreover, we were not able to define whether AF was present before hospitalization or detected during hospital stay, and whether it was paroxysmal, persistent or permanent. Furthermore, we included in the analysis only patients who were admitted to hospital; therefore, the number of cases and mortality rate could have been underestimated, due to the missing of patients with ICH rapidly deteriorated and dead in the setting of Emergency Departments, where compilation of hospital discharge records is not mandatory. Our study lacks a detailed analysis about co-morbidities in patients with AF-related ICH, and about the role of anticoagulants on poor outcome. Moreover, our study lacks a long-term follow-up; therefore, it could have underestimated the real burden of prevalence and mortality. Finally, our study does not provide information about the reasons of the reduced mortality over the years, such as the role of reversal therapy in coagulopathy-related ICH in AF. Despite these limitations, we think that our data could contribute to the knowledge of the relationship between spontaneous ICH and AF.
CONCLUSION
In patients with spontaneous ICH the burden of AF is absolutely not negligible, and seems to be increasing over the years. Further prospective studies are warranted.
REFERENCES
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, et al. (2016). ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur J Cardiothorac Surg. 50: e1-e88.
- Qureshi AI, Mendelow AD and Hanley DF. (2009). Intracerebral haemorrhage. Lancet. 373: 1632-1644.
- McGrath ER, Kapral MK, Fang J, Eikelboom JW, et al. (2012) Investigators of the Registry of the Canadian Stroke Network.. Which risk factors are more associated with ischemic stroke than intracerebral hemorrhage in patients with atrial fibrillation? Stroke. 43: 2048-2054.
- Horstmann S, Rizos T, Jenetzky E, Gumbinger C, et al.(2014). Prevalence of atrial fibrillation in intracerebral hemorrhage. Eur J Neurol. 21: 570-576.
- D'Amore C, Paciaroni M, Silvestrelli G, Agnelli G, et al. (2013). Severity of acute intracerebral haemorrhage, elderly age and atrial fibrillation: independent predictors of poor outcome at three months. Eur J Intern Med. 24: 310-313.
- Go AS, Hylek EM, Phillips KA, Chang Y, et al. (2001). Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA. 285: 2370-2375.
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, et al. (2006). Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 114: 119-125.
- Heeringa J, van der Kuip DAM, Hofman A, Jan A. Kors, et al. (2006). Prevalence, incidence, and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J. 27: 949-953.
- Ogilvie IM, Newton N, Welner SA, Cowell W, et al. (2010). Underuse of oral anticoagulants in atrial fibrillation: a systematic review. Am J Med. 123: 638-645.
- Huhtakangas J, Tetri S, Juvela S, Saloheimo P, et al. (2011). Effect of increased warfarin use on warfarin-related cerebral hemorrhage: a longitudinal population-based study. Stroke. 42: 2431-2435.
- Dequatre-Ponchelle N, Henon H, Pasquini M, Rutgers MP, et al. (2013). Vitamin K antagonists-associated cerebral hemorrhages: what are their characteristics? Stroke. 44(2): 350-355.
- Schols AM, Schreuder FH, van Raak EP, Schreuder TH, et al. (2014). Incidence of oral anticoagulant-associated intracerebral hemorrhage in the Netherlands. Stroke. 45: 268-270.
- Flaherty ML, Kissela B, Woo D, et al. (2007). The increasing incidence of oral anticoagulant-associated intracerebral haemorrhage. Neurology. 68: 116-121.
- Masotti L, Di Napoli M, Godoy DA, Lorenzini G, et al. (2016). Intracerebral hemorrhage score in patients with spontaneous intracerebral hemorrhage pretreated and not treated with antithrombotics. Neurology and Clinical Neuroscience. 4: 169-175.
- Cucchiara B, Messe S, Sansing L, Kasner S, et al. (2008). Hematoma growth in oral anticoagulant related intracerebral hemorrhage. Stroke. 39: 2293-2296.