Previous Issues Volume 2, Issue 1 - 2017
Bilateral Stress Fractures of Pubic Ramus in a Patient affected by Hyperparathyroidism
Güzelali Özdemir1 , Enver Kılıç1 , Kemal Andıç1 , Alper Deveci1*
1Ankara Numune Research and Training Hospital, Orthopaedics and Traumatology Clinic, Altindag, Ankara, Turkey.
Corresponding Author: Alper Deveci, Ankara Numune Research and Training Hospital, Orthopaedics and Traumatology Clinic, Altindag, Ankara, Turkey, Tel: 90 312 508 40 00; E-Mail: [email protected]
Received Date: 27 Jan 2017 Accepted Date: 14 Feb 2017 Published Date: 20 Feb 2017
Copyright © 2017 Deveci A
Citation: Deveci A, Özdemir G, Kılıç E and Andıç K. (2017). Bilateral Stress Fractures of Pubic Ramus in a Patient Affected by Hyperparathyroidism. Mathews J Case Rep 2(1): 026.
ABSTRACT
This case report presents a 48-year-old patient who was diagnosed of bilateral pubic ramus stres fracture in one year period. She was admitted with hip and groin pain. In our case, direct radiography followed by MRI was used for diagnosis. Hyperparathyroidism was detected as a etiological cause. Patient underwent conservative treatment for bilateral stres fractures of pubic ramus with perfect results. Attending to this case report, in patients with non-traumatic groin pain and endocrinological disorders, pubic ramus stress fracture is a diagnosis that should be kept in mind.
INTRODUCTION
Stress fractures are those that occur in a local area of a normal or pathologic bone, due to less powerful forces that will normally result in a complete fracture. This kind of fractures are divided into three different subgroups: fatigue fracture, insufficiency fracture, and pathologic fracture. Fatigue fractures occur in healthy bones due to unusual mechanical effect. Their prevalency is increased in young adults, especially in weight bearing bones. Attending to the risk factors, fatigue fractures are most frequenly observed in athletes, dancers, and soldiers [1]. On the other hand, insufficiency fractures occurs as a result of reduced bone resistance under normal bearing [2]. Many clinical risk factors have been identified with this fracture type, including osteoporosis, osteomalacia, hyperparathyroidism, rheumatoid arthritis, long term use of cortisone, diabetes mellitus, fibrous dysplasia, renal insufficiency, and radiotherapy [3]. Attending to insufficiency fractures, most pelvic insufficiency fractures occur in women, particularly those with osteoporotic bone. They represent, approximately, 1-2% of all the stress fractures, and they most commonly observed at the pubic ramus [4-6]. This kind of fractures are usually asymptomatic; nevertheless, these patients ay present groin and back pain [7]. For our knowledge, bilateral pubic ramus stress fracture due to hyperparathyroidism has not been reported previously. In this case report, we present a case report of a female patient affected of this type of fracture and realize a short review about of stress fractures in patients affected of endocrinological mineral balance disorders, including hyperparathyroidism.
CASE REPORT
A 48 years-old female patient was admitted to our polyclinic affected by right hip and groin pain for two months without trauma history. The symptomatology increased with daily activities and effort, however, it decreased with rest. Attending to her personal history, the patient did not present any illness during this period of time, she was not under treatment with steroids, and she was no under radiation exposure. Duirng this period, the patient was under treatment with non-steroid antiinflammatory drug (NSAID) without beneficial results. Due to that reason, she applied to our polyclinic several times during the last two months. Attending to the physical exploration, an antalgic gait was observed, but the patient did not need assistance devices to walk. There was not observed swelling, tenderness, warmth or color disturbs at right hip level. There was not also showed range of motion (ROM) limitation at the hip joint. However, the patient reported pain duringhip joint movements. Lasegue test as well as sensorial exploration on lower extremities did not showed any disturbs. According to the physical exploration, a pelvic x-radiograph study was requested showing a right pubic ramus stress fracture (Figure 1).

Figure 1: Radiograph showing right superior and inferior stress fracture.
A pelvic magnetic resonance imaging (MRI) was realized to complete the study observing edematous changes due to a fracture at right superior and inferior pubic ramus (Figure 2).
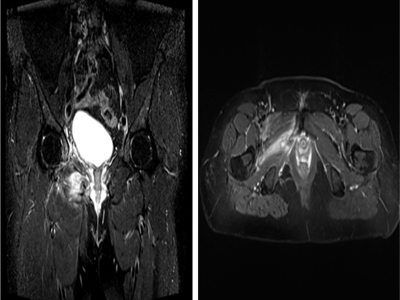
Figure 2: Figure 2: MRI image showing edematous changes and fracture at right superior and inferior pubic ramus.
Attending to these results, a blood test was realized. Results showed that blood count, C-reactice protein (CRP), rheumatoid factor (RF), calcium, phosphorus, alkhaline phosphatese, vitamine D, parathyroid hormone (PTH) levels and bone mineral density (BMD) tests were normal. The patient was discharged with the diagnosis of right pubic ramus stress fracture and followed up monthly. Six months later, pelvic x-radiograph was realized observing that right pubic ramus stress fracture was healed (Figure 3). The patient reportedthat she did not show any complaint with daily activities and physical effort.

Figure 3: Six months later, radiograph showedhealed right superior and inferior pubic ramus stres fractures.
Six months later, she was admitted to our polyclinic again with left hip joint and groin pain. Her pain was increasing with daily activities and effort but decreasing with rest, like one year ago. Antalgic gait started again. A pelvic radiograph was requested observing a left pubic ramus fracture (Figure 4). She did not report trauma history. To complete the study, a MRI was requested showing edematous changes and fracture at left inferior pubic ramus level. As a result, left pubic ramus stress fracture was diagnosed (Figure 5). Motion restriction and resting were offered as a treatment.

Figure 4: Radiograph showing left inferior pubic ramus stress fracture.
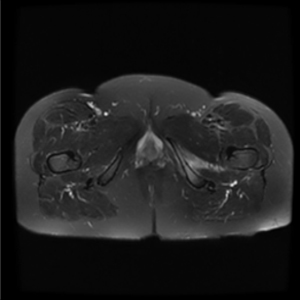
Figure 5: MRI image showing edematous changes and fracture at left inferior pubic ramus.
Blood count, CRP, RF, calcium, phosphorus, alkhaline phosphatese, vitamine D, and PTH levels, and BMD tests were requested again. Vitamine D level was 3.3 ng/mL (range 20-50 ng/mL). Vitamine D replacement was started. PTH level was 106,5 pg/mL (normal range 10-55). Patient was followed up with monthly controls. Two months later vitamine D level was 32 ng/mL and PTH level was 128 pg/mL. A parathyroid ultrasound image was used to check parathyroid glands showing a bilateral parathyroid adenom. Attending to these results, a parathyroid scintigraphy was realized to complete the study previously to the surgery (Figure 6).
Figure 6: Scintigraphy image showing bilateral parathroid.
One month later, the adenoma was removed with bilateral parathyroidectomy. After the operation, PTH level was 43 pg/mL, and four months later, left inferior pubic ramus was healed (Figure 7). There was no pain with daily activities and physical effort.

Figure 7: Four months later, radiography showed healed left inferior pubic ramus stres fracture.
DISCUSSION
Insufficiency fractures occur when normal forces are applied to weakened bones with reduced elastic resistance. This kind of fractures are usually observed in older women with postmenopausal osteoporosis. In 1937 Wachsmuth described in first time pubic ramus stress fractures [8]. Pelvic stress fractures represent approximately 1% to 2% of all stress fractures, and are most frequently observed in pubic rami level [5-7,9]. This kind of fractures may appear asymptomatic or presenting hip or groin pain [4, 10]. Due to that,clinical diagnosis may be delayed, especially in patients affected by groin pain without history of trauma, because of the symptoms may be attributed to coexisting arthritis or degenerative disease. Clinical treatment decisions are based on patient's history, clinical examination and imaging tests. Radiography studies lack the ability to determine acute stress fractures because of it may take 3 weeks for cortical irregularities and periosteal reactions to become evident. Therefore, other imaging techniques are recommended [10-12]. Direct radiography's sensivity is 37% in diagnosis of stress fractures, andthis may be the reason why a stres fracture could be underdiagnosed [13]. Regardless of stress fracture location, MRI is currently the gold standard, largely due to the instrument's ability to display both soft tissue and bone edema [14]. One of the earliest signs of stress fracture is bony edema, which is not easily visible on standard radiographic imaging [15]. In our case, direct radiography followed by MRI was used for diagnosis. There are a lot of case reports about insufficiency pubic ramus fracture. However bilateral pubic ramus insufficiency fracture is rare, such as after total hip arthroplasty [16]. Reveiweing the literature, we did not observed a case report of bilateral pubic ramus insufficiency fracture in a patient affected ofendocrinological disorders. For our knowledge, this is the first case reported in the literatureof a bilateral pubic ramus insufficiency fracture is a patient affected of hyperparathyodisim. Treatment of stress fractures is aimed at balancing bone destruction and and new bone formation. The easiest way to reduce bone destruction is removing the stressors. Because of that, most of this kind of fractures may be healed with immobilization [17]. Surpringsly, some experimental studies have observed that NSAIDs may slow the recovery of stress fractures [18, 19]. However, more studies are needed to improve the knowledge of the adequate management of these fractures.
CONCLUSION
Pelvic stress fractures are frequently overlooked fractures in clinic. In patients with non-traumatic groin pain and endocrinological disorders, pubic ramus stress fracture is a diagnosis that should be kept in mind. The purpose of this case report is to remind us the diagnosis of stress fracture in patients with pain and endocrinological mineral balance disorders such as hyperparathyroidism.
REFERENCES
- Pentecost RL, Murray RA and Bridnley HH. (1964). Fatigue, insufficiency and pathologic fractures. JAMA. 187: 1001-1004.
- Daffner RH and Pavlov H. (1992). Stres fractures: Currentconcepts. Am J Radiol. 159: 245-252.
- Weber M, Hasler P and Gerber H. (1993). Insufficiencyfracture of thesacrum. Twentycasesandreview of theliterature. Spine (PhilaPa 1976). 18: 2507-2512.
- Hosono M, Kobayshi H and Fujimoto R. (1997). MRI appearance of parasymphseal insufficiency fractures of pubis. SkeletRadiol. 26: 525-528.
- Lappe J, Davies K and Recker R. (2005). Quantitative ultrasound: use in screening for susceptibility to stress fractures in female army recruits. J Bone Miner Res. 20(4): 571-578.
- O’Brien T, Wilcox N and Kersch T. (1995). Refractory pelvic stress fracture in a female long-distance runner. Am J Orthop (Belle Mead NJ). 24(9): 710-713.
- Hershman EB, Lombardo J and Bergfeld JA. (1990). Femoral shaft stress fractures in athletes. Clin Sports Med. 9(1): 111-119.
- Stechow M. (1937).Fussödem und röntgen strahlen. Deutsche Militärärztliche Zeitschrift. 26: 465.
- Peh WC. (2001). Clinics in diagnostic imaging insufficiency fractures of the pelvis. Singapore Med J. 42(4): 183-186.
- Lapp JM. (2000). Pelvic stress fracture: Assessment and risk factors. J Manipulative Physiol Ther. 23: 52-55.
- McCormick F, Nwachukwu BU and Provencher MT. (2012). Stress fractures in runners. Clin Sports Med. 31(2): 291-306.
- Spitz DJ and Newberg AH. (2002). Imaging of stress fractures in the athlete. Radiol Clin North Am. 40(2): 313-331.
- Kiuru MJ, Pihlajamaki HK and Ahovuo JA. (2003). Fatigue stress injuries of the pelvic bones and proximal femur: Evaluation with MR imaging. Eur Radiol. 13: 605-611.
- Boden BP and Osbahr DC. (2000). High-risk stress fractures: evaluation and treatment. J Am Acad Ortop Surg. 8(6): 344-353.
- Delvaux K and Lysens R. (2001). Lumbosacral pain in an athlete. Am J Phys Med Rehabil. 80(5): 388-391.
- Hayashi T, Nishiyama T and Fujishiro T. (2012). Bilateral insufficiency fracture of the pelvis following THA: a case report, Case Reports in Medicine.
- Behrens SB, Deren ME and Matson A. (2013). Stress fractures of the pelvis and legs in athletes: A review. Sports Health. 5: 165-174.
- Li M, Healy DR and Li Y. (2005). Osteopenia and impaired fracture healing in aged EP4 receptor knockout mice. Bone. 37: 46-54.
- Krischak GD, Augat P and Blakytny R. (2007). The non-steroidal anti-inflammatory drug diclofenac recudes appearance of osteoblasts in bone defect healing in rats. Arch Orthop Trauma Surg. 127: 453-458.