Current Issue Volume 6, Issue 1 - 2024
Atypical Aneurysmal Bone Cyst of Humerus with Pathological Fracture Mimicking a Malignancy - A Case Report
Pranav Kothiyal1,*, Kunal Vij2, Arnav Pathak3
Associate Professor, Department of Orthopaedics, SGRRIMHS, Dehradun, Uttarakhand, India
Professor, Department of Orthopaedics, SGRRIMHS, Dehradun, Uttarakhand, India
Junior Resident, Department of Orthopaedics, SGRRIMHS Dehradun, Uttarakhand, India
*Corresponding Author: Pranav Kothiyal, Associate Professor, Department of Orthopaedics, SGRRIMHS, Dehradun, Uttarakhand, India; Email: [email protected]
Received Date: May 20, 2024
Publication Date: June 17, 2024
Citation: Kothiyal P, et al. (2024). Atypical Aneurysmal Bone Cyst of Humerus with Pathological Fracture Mimicking a Malignancy - A Case Report. Orthop Res J. 6(1):26.
Copyright : Kothiyal P, et al. © (2024)
ABSTRACT
We present a case of an atypical aneurysmal bone cyst (ABC) of the humerus in a 14-year-old male patient who presented with a pathological fracture. Initially suspected as a malignancy due to its aggressive radiological features, the diagnosis was challenging. Management of the fracture by closed intramedullary nailing followed by histopathological examination of the aspirate from the reamer confirmed the lesion as an atypical ABC. This case underscores the importance of considering atypical presentations of benign lesions in the differential diagnosis of bone tumors to avoid unnecessary aggressive treatments.
INTRODUCTION
Aneurysmal bone cysts (ABCs) are benign bone lesions commonly occurring in the metaphysis of long bones, characterized by expansive, cystic, and hemorrhagic lesions. Aneurysmal bone cysts have an annual prevalence of 0.14 - 0.32 per 100,000 population [1,2] and comprises about 2.5% of all bone tumors [3]. It has an equal distribution among male and female patients [4,5], and most commonly is seen in skeletally immature patients especially in the first two decades of life. However, sometimes atypical presentations of ABCs may pose diagnostic challenges, rarely mimicking malignant bone tumors. Here, we report a case of an atypical ABC of the humerus presenting with a pathological fracture.
CASE PRESENTATION
A 16-year-old male patient garage worker by occupation presented with sudden onset pain and swelling in the right arm following a minor trauma during work.
The patient gave history of mild nonspecific generalised pain in his right arm since past 8 months.
On examination diffuse swelling was appreciated at the junction of mid and distal third of right arm.
Abnormal mobility was not elicited as the part was tender on palpation. The overlying skin above the swelling was normal in texture. It was not tethered to any underlying structures and didn't show any signs of dilated veins or fungation. The patient was evaluated by getting plain X-rays of the arm done.
Radiographic imaging revealed an osteolytic lesion with cortical destruction in the proximal diaphysis of the right humerus associated with a pathological fracture.
Magnetic resonance imaging (MRI) depicted a expansile altered signal intensity lesion with endosteal scalloping, cortical thinning and a narrow zone of transition involving mid-diaphyseal region. Cortical defect was visualised along with adjacent soft tissue edema.
MANAGEMENT
Given the somewhat aggressive radiological features of the lesion and pathological fracture, the patient underwent surgical management in the form of closed intramedullary nailing of humerus and histopathological examination of the aspirate obtained on reaming of the medullary canal.
The histopathological examination revealed characteristic features of an aneurysmal bone cyst, including cavernous spaces filled with blood, fibrous septa, and osteoclast-like giant cells, confirming the diagnosis of an atypical ABC.
Postoperative period was uneventful and the lytic lesion gradually resolved over subsequent months and the fracture united. The patient achieved full range of movements at the shoulder and elbow and has resumed his routine activities after 8 months of surgery.
Serial imaging during every follow up showed progressive healing of the fracture site and regression of the cystic lesion. At 12 months post-surgery the recovery is satisfactory without evidence of any recurrence or complications.
DISCUSSION
Atypical presentations of ABCs, particularly with pathological fractures and aggressive radiological features, may closely mimic malignant bone tumors, posing diagnostic dilemmas.
ABCs have a predilection to afflict young patients and is diagnosed more commonly in the second decade of life as was the case with our patient [3].
The location of Aneurysmal bone cysts is usually metaphyseal [6-8] but this patient had the lesion in humeral diaphysis that made the diagnosis confusing. The management of such cases requires a multidisciplinary approach involving orthopedic surgeons, radiologists, and pathologists who can help in making the diagnosis accurately and minimise the chances of error and hence the correct treatment approach. Curettage of the lesion with bone grafting remains the primary treatment modality in most cases of a aneurysmal bone cyst [9]. However in this case indirect curettage of the lesion by reamer and relative stability provided by the nail without any bone graft proved to be sufficient for the lesion to resolve and the fracture healing to occur.
During the placement of the intramedullary nail the undisplaced fracture got slightly displaced increasing our apprehensions regarding consolidation at the lesion and spontaneous union of the fracture.
However improved radiological picture depicting increased mineralisation at fracture site and signs of union at 2 months post-surgery laid our worries to rest.
Local recurrence rate of ABCs after curettage and grafting is about 11.8% - 30.8% [10,11] which can occur even upto two years after the surgery. Due to this fact prolonged follow up is required in histopathologically aggressive lesions to rule out any recurrence. Our patient was followed up every two months till one year without any sign of recurrence.
Awareness of atypical variants of ABCs and meticulous histopathological examination are crucial for accurate diagnosis and appropriate management, thereby avoiding unnecessary aggressive treatments.
CONCLUSION
This case highlights the diagnostic challenges posed by atypical presentations of benign bone lesions, such as ABCs, which may mimic malignant tumors. Clinicians should maintain a high index of suspicion for atypical variants of ABCs in patients presenting with aggressive radiological features and pathological fractures. Timely diagnosis and appropriate management are paramount for achieving favorable outcomes.

Figure 1: Preop xray of the patient showing a expansile lytic lesion in humerus diaphysis with pathological fracture.
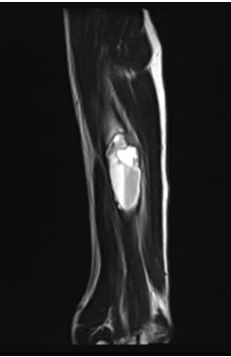
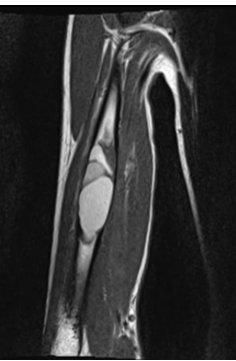
Figure 2: Pre-op MRI showing expansile lytic lesion in the mid humerus with altered signal intensity and cortical breach.

Figure 3: Immediate post op
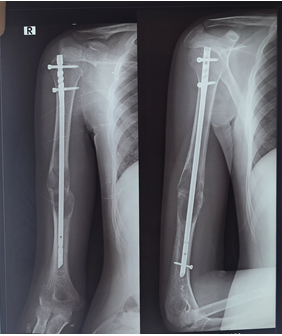
Figure 4: xray at 2 months post op
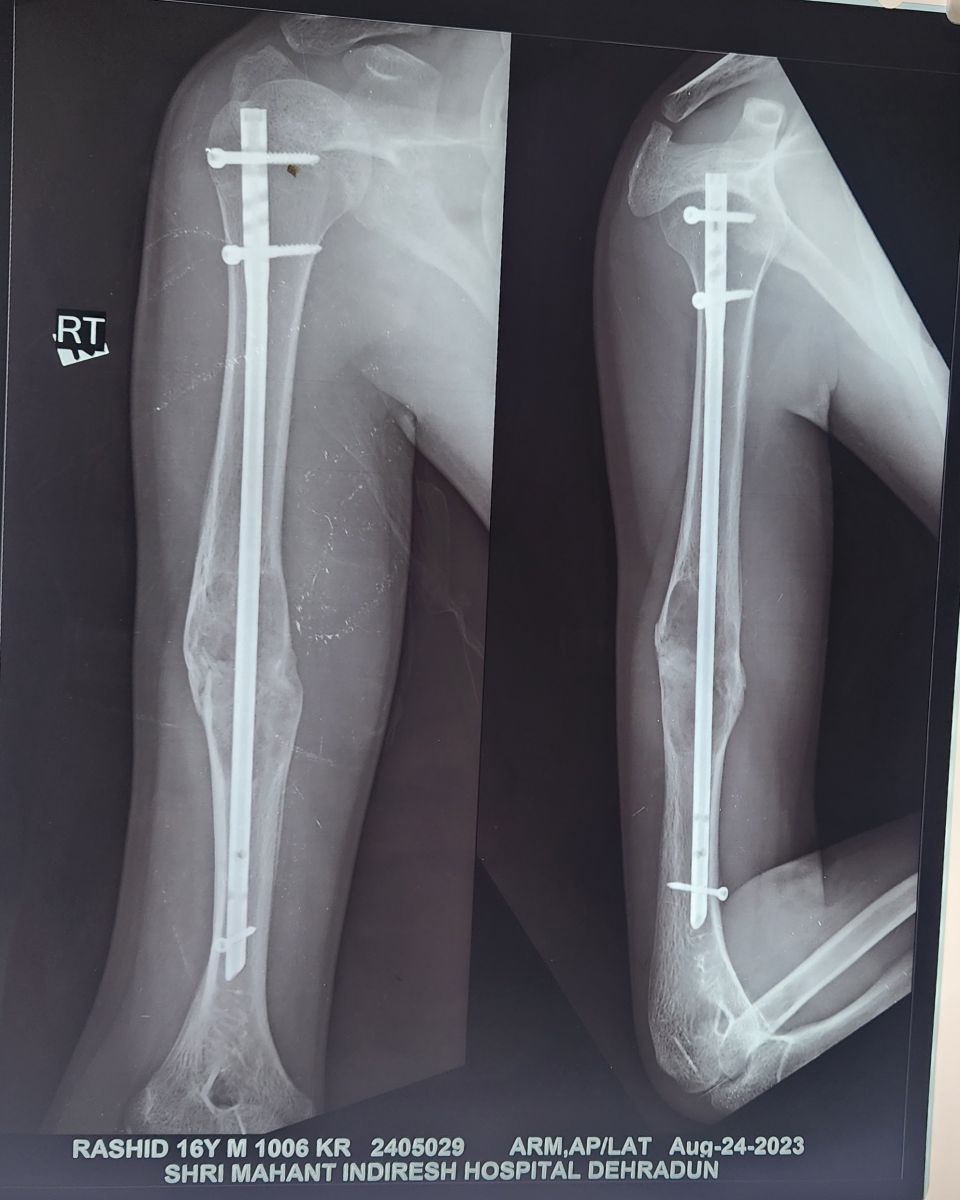
Figure 5: Xray at 9 months post op
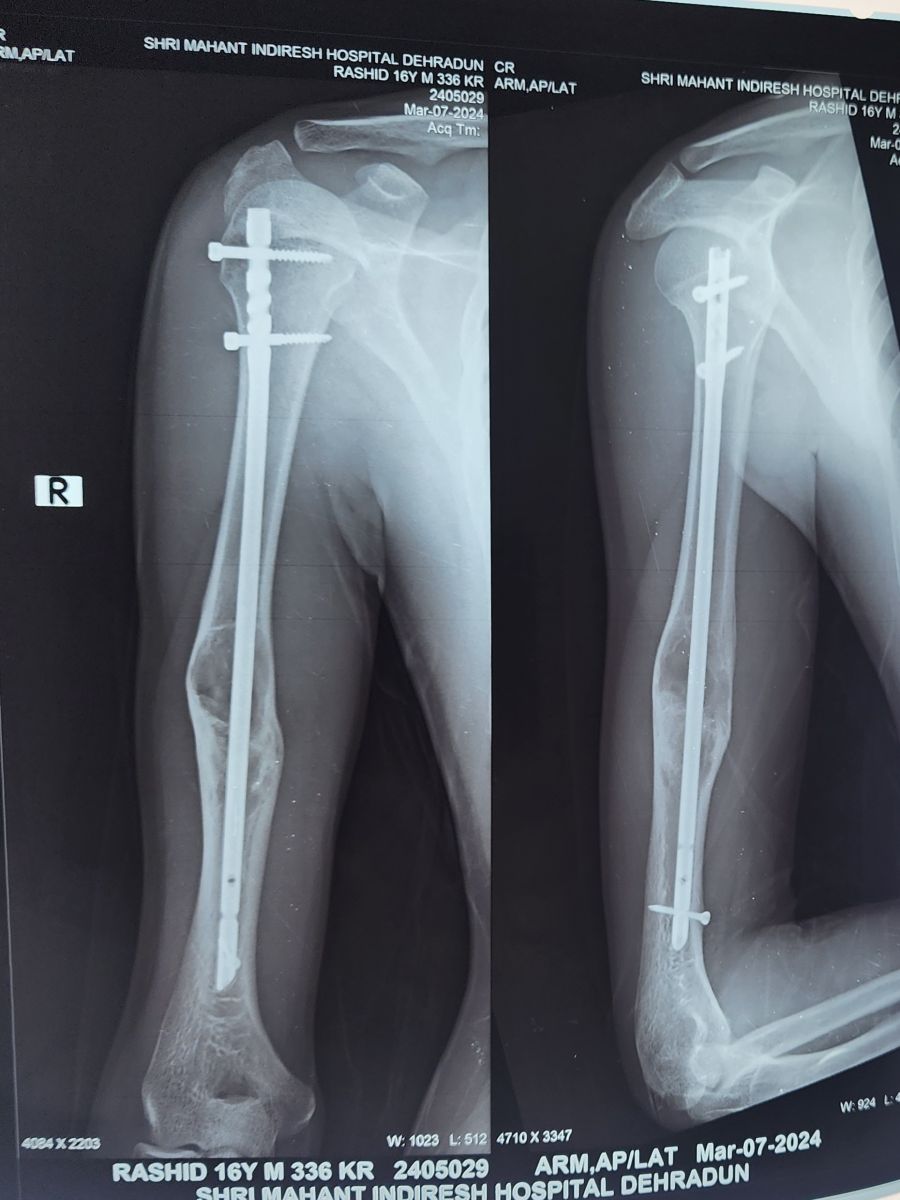
Figure 6: Xray at 11 month post op
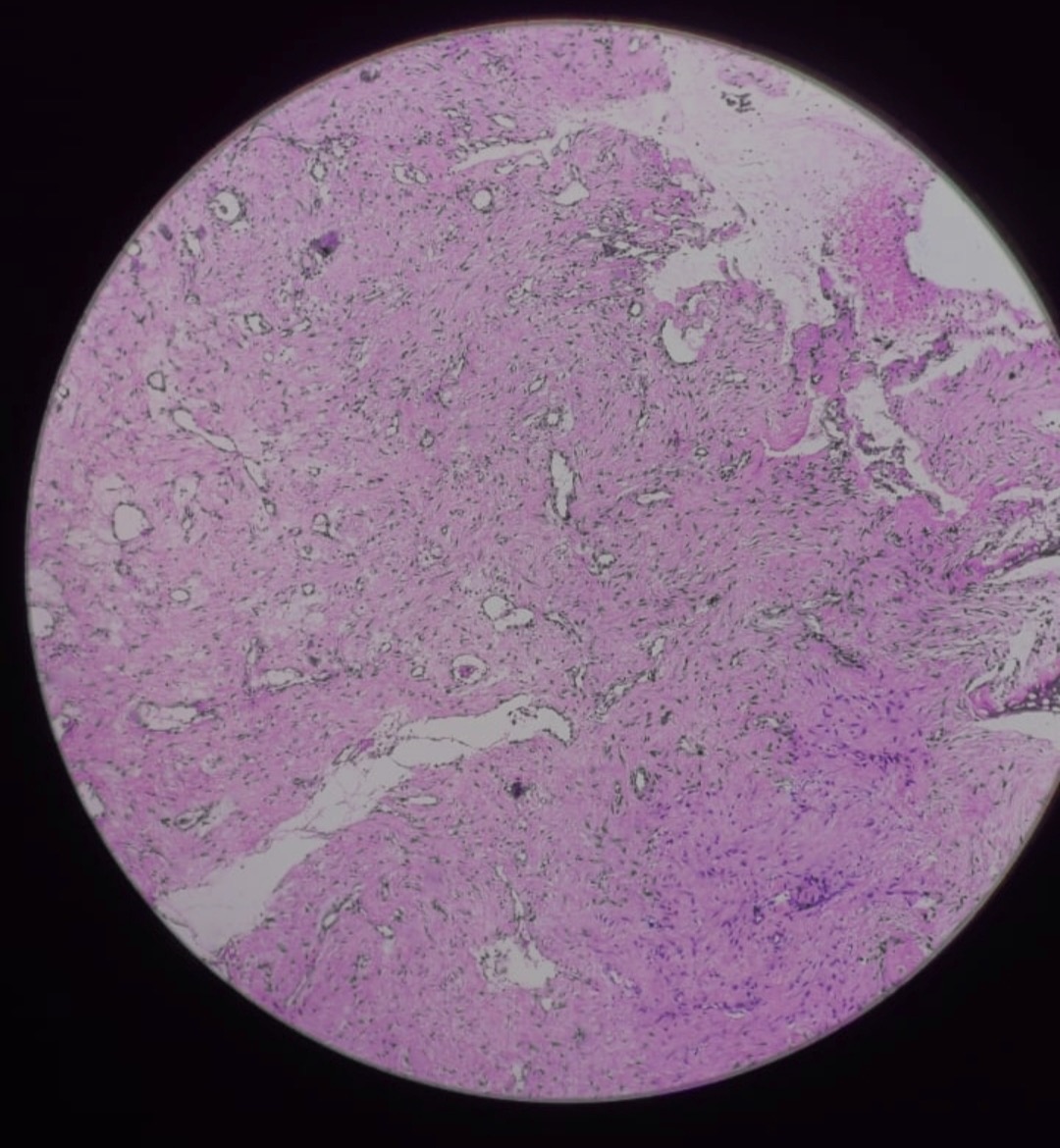
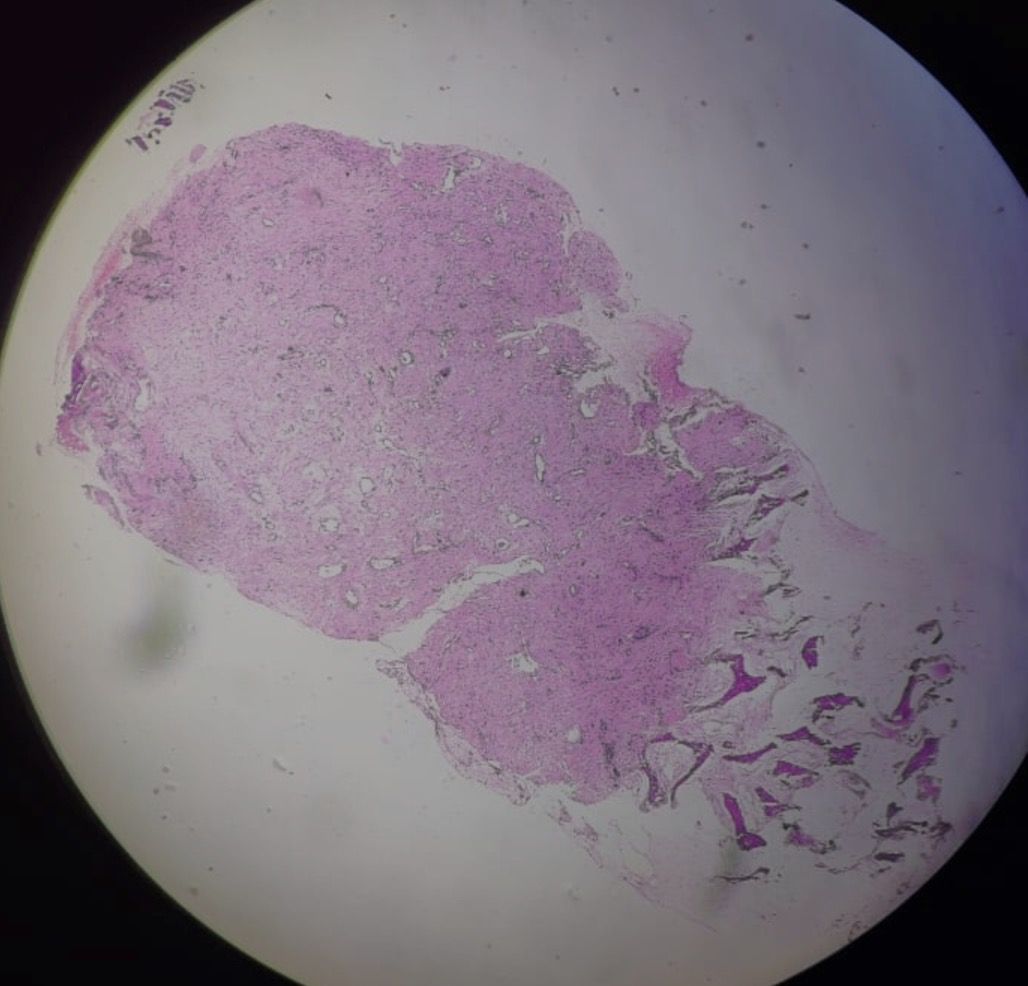
Figure 7: Histopathological examination showing multiple cystic spaces, some blood filled, with a portion of cyst wall with scattered giant cells with no significant atypia consistent with the diagnosis of aneurysmal bone cyst
REFERENCES
- Zehetgruber H, Bittner B, Gruber D, Krepler P, Trieb K, Kotz R, et al. (2005). Prevalence of aneurysmal and solitary bone cysts in young patients. Clin Orthop Relat Res 439:136–143.
- Czerniak B. (2015). Dorfman and Czerniak’s bone tumors, E-Book. 2nd. Philadelphia: Elsevier Health Sciences.
- Leithner A, Windhager R, Lang S, Haas OA, Kainberger F, Kotz R. (1999). Aneurysmal bone cyst: a population based epidemiologic study and literature review. Clin Orthop Relat Res. 363:176–179.
- Vergel De Dios AM, Bond JR, Shives TC, McLeod RA, Unni KK. (1992). Aneurysmal bone cyst: a clinicopathologic study of 238 cases. Cancer. 69:2921–2931.
- Martinez V, Sissons HA. (1988). Aneurysmal bone cyst: a review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer. 61:2291–2304.
- Ruiter DJ, van Rijssel TG, van der Velde EA. (1977). Aneurysmal bone cysts: a clinicopathological study of 105 cases. Cancer. 39(5):2231-2239.
- Martinez V, Sissons HA. (1988). Aneurysmal bone cyst: a review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer. 61(11):2291-2304.
- Yu GV, Roth LS, Sellers CS. (1998). Aneurysmal bone cyst of the fibula. J Foot Ankle Surg. 37(5):426-436.
- Campanacci M, Capanna R, Picci P. (1986). Unicameral and aneurysmal bone cysts. Clin Orthop. 204:25-36.
- Schreuder HW, Veth RP, Pruszczynski M, Lemmens JA, Koops HS, Molenaar WM. (1997). Aneurysmal bone cysts treated by curettage, cryotherapy and bone grafting. J Bone Joint Surg Br. 79(1):20-25.
- Vergel De Dios AM, Bond JR, Shives TC, McLeod RA, Unni KK. (1992). Aneurysmal bone cyst: a clinicopathologic study of 238 cases. Cancer. 69(12):2921-2931.