Previous Issues Volume 1, Issue 3 - 2016
Assessing Patient Safety Culture in an Emergency Department
Philippe Leveau
SMUR Urgences, Centre Hospitalier Nord Deux Sevres, 79103 Thouars Cedex, France.
Corresponding Author: Philippe Leveau, SMUR Urgences, Centre Hospitalier Nord Deux Sevres, 79103 Thouars Cedex, France. Tel: 04 3275 3181; E-Mail: [email protected]
Received Date: 30 May 2016
Accepted Date: 03 Sep 2016
Published Date: 15 Sep 2016
Copyright © 2016 Leveau P
Citation: Leveau P. (2016). Assessing Patient Safety Culture in an Emergency Department. Mathews J Emergency Med. 1(3): 015.
ABSTRACT
Introduction: The culture of safety has an impact on the quality of care. It was measured in an emergency department. Method: The French translation of the Hospital Survey on Patient Safety Culture was used with all the medical and nonmedical staffs of the ED. Results: The rate of participation was equal to 83 %. Only 50 % of the referees had a positive overall perception of patient safety. There was 60 % of positive answers for reporting events, 82% for supervisor expectations and actions promoting safety, 59 % for organizational learning continuous improvement, 86 % for teamwork in the department, 67 % for the communication openness, 49 % for the nonpunitive response to error, 39 % for the human resources, 32 % for the hospital management support for patient safety and 47 % for the teamwork across hospital units. Discussion: These results are in accordance with the literature, except the clearly upper rate of participation. The dimensions of the culture of safety which overtake the perimeter of the emergency department have the worst scores, highlighting a strategic deficit of establishment. The positive points are the excellent scores for teamwork in the department and supervisor expectations and actions promoting safety. They are an asset for implementation of corrective measures. Conclusion: These results allow us to set up targeted measures of improvement, in particular an anonymous system of reporting events and errors reversed forecast to a system of distribution between the actors.
KEYWORDS
Safety Management; Patient Safety; Safety Culture; Emergency Medicine; Emergency Department.
INTRODUCTION
Safety of care is a public health priority. There are in France 2.6 serious adverse events (AEs) preventable 1,000 patientdays, between 120 and 190,000 preventable AEs during hospitalization each year [1]. In addition to the solutions adopted as new regulatory texts, development of standards and the assessment and training of professionals, safety culture of care allows a collective awareness to make the safety of care a priority. In other words, it allows each professional to always have in mind the question of the impact of its decisions and actions on the safety of care. Because emergency medicine is a risky activity, the culture of safety was estimated from the different actors of the Emergency Department (ED). There are several tools to measure safety culture of care [2]. The French translation of the Hospital Survey On Patient Safety Culture (HSOPSC) [3] recommended by the french Haute Autorite de Sante [4] was used. This questionnaire has been validated in several other countries [5-10]. It allows to estimate the safety culture of care across ten dimensions (Table 1). This has given us paths for action to improve the safety of care.
Table 1: dimensions of safety culture and their definition.
|
Dimension |
Definition |
|
Global safety perception |
Safety of care is never neglected in favor of a larger performance, operation and service procedures can prevent the occurrence of errors and there are few problems relating to the safety of care in the service. |
|
Adverse events and errors reports |
The following errors are reported: those detected and corrected before affecting the patient, those who do not have the potential to harm the patient, those that can harm the patient but ultimately have no effect |
|
Relationships with supervisors |
Superiors congratulated the staff when the work is done in compliance with safety rules, consider staff suggestions for improving the safety of care, do not neglect security when working faster and neglect not recurrent problems of safety of care |
|
Learning organization and continuous improvement of service (feedback) |
The staff is informed of errors occurred, receives feedback on the measures taken, and discusses the resources available to prevent errors. Errors lead to positive changes and the effectiveness of these changes is evaluated. |
|
Teamwork in the ED |
In the ED, the persons support each other, treat each other with respect and work in teams. Together, they improve their security practices of care. |
|
Freedom of expression |
The staff speak freely if he sees something that can harm a patient and do not hesitate to question the hierarchy. |
|
Not repression of error |
The staff did not feel that his errors and alerts are against him, or that his errors are noted in the administrative records. |
|
Human resources |
There are enough staff to the workload, the number of hours worked is adapted for the highest quality of care and the staff did not try to do too much too quickly. |
|
Safety management |
Management establishes a work environment that promotes safety of care. It is not interested in security only after an adverse event occurred and actions shows that safe care is the first priority. The hospital services work together to provide patients with the best care. |
|
Teamwork between departments |
Hospital departments shall cooperate and coordinate in order to provide patients with quality care. It is rarely unpleasant to work with staff from other services. There are rarely problems when important information regarding patient care is transmitted between services and during shift changes. |
METHOD
All medical, nursing and administrative member of the ED were asked to complete the French version of HSOPSC in February 2013 [11]. The weighting of items was changed with a Likert scale pair. Each questionnaire was anonymous. The statistical significance was set at 0.05. Confidence intervals were calculated by the method of the ellipse through a computer on Internet [12].
RESULTS
The ED included 106 agents in total during the study across three geographical locations (Thouars, Parthenay Bressuire), each grouping mobile intensive care unit, emergency rooms and short-term hospitalization unit. The average response rate was equal to 83%, with no statistically significant difference between professions (X2 = 3.51, p > 0.20) or between sites (X2 = 2.13, p > 0.30) (Table 2). Seniority in the job was equal to (mean ± SD) 11 ± 5 years (ambulance being younger, F4,78 = 12.21, p < 0.01), seniority in the same establishment 8 ± 3 years (emergency physicians EP being younger, F4,78 = 14.53, p < 0.01) and age in the emergency center equal to 8 ± 4 years (EP being the youngest F4,78 = 9.10, p < 0.01).
Table 2: survey characteristics (ED: emergency department, AEs: adverse events, total number of participants: 88).
| Emergency physicians | Nurses | Carers | Ambulances | Administrative | |
| Number | 24 | 30 | 16 | 13 | 5 |
| Seniority: in ED | 7±4 | 7±4 | 8±3 | 8±4 | 3±2 |
| in profession | 11±4 | 10±5 | 12±3 | 9±5 | 7±4 |
| in hospital | 7±4 | 8±3 | 10±2 | 8±4 | 3±1 |
| Involvement in structure or risk management committees | Y e s | No | |||
| 12 | 76 | ||||
| Nb AEs reported last year | 0 | 01-Feb | 03-May | 06-Oct | > 10 |
| 42 | 27 | 13 | 0 | 1 | |
| Working time | 0.5 | > 50% | Response rate of participants | Response rate of items | |
| Number | 5 | 83 | 83% | 99% | |
The mean response rate of each items was equal to 99 ± 1.3%. The number of AEs reported during the past 12 months is very low, equal to 1.1 ± 1.4, comparable between jobs (F4,78 = 1.37, p > 0.05) and between sites (F3,85 = 1.57, p > 0.05). 50% of agents surveyed reported no adverse events in the previous year. Results was examined in their entirety, then comparing sites, jobs and seniority (Table 3).
Table 3: percentages of positives responses to different dimensions of safety of care culture in the global emergency department, between sites, between professions (EP: emergency physician) and between seniority in the job (in bold, statistical significant values with p < 0.05).
| Global | Comparison between sites | Comparison between professions | Comparison seniority in the job | |||||||
| Thouars | Bressuire | Parthenay | EP | Nurses | Carers | Ambulanes | = 5 years | > 5 years | ||
| Overall perception of safety | 50 | 65 | 36 | 45 | 50 | 45 | 42 | 63 | 59 | 42 |
| Adverse events and errors reports | 60 | 58 | 56 | 68 | 44 | 56 | 67 | 92 | 68 | 45 |
| Relationships with supervisors | 82 | 84 | 76 | 87 | 85 | 84 | 70 | 88 | 89 | 80 |
| Feedback | 59 | 69 | 44 | 64 | 59 | 57 | 43 | 75 | 72 | 48 |
| Teamwork in the ED | 86 | 89 | 78 | 91 | 82 | 93 | 79 | 83 | 89 | 82 |
| Freedom of expression | 67 | 70 | 56 | 74 | 69 | 66 | 60 | 67 | 72 | 63 |
| Not repression of error | 49 | 52 | 40 | 53 | 44 | 52 | 45 | 49 | 57 | 45 |
| Human resources | 39 | 44 | 36 | 32 | 31 | 40 | 38 | 49 | 39 | 32 |
| Safety management | 32 | 36 | 27 | 32 | 32 | 27 | 32 | 33 | 48 | 20 |
| Teamwork between departments | 47 | 49 | 45 | 46 | 49 | 45 | 40 | 55 | 58 | 40 |
Global Results
The direct assessment showed a Gaussian distribution quotes (Figure 1) with a mean value equal to 5.3 ± 2.1 on 10. HSOPSC explores the culture of safety in ten dimensions, each evaluated by 3-6 different issues. They are the overall perception of safety (50% positive response, confidence interval 95% (CI95: 40-60), frequency of reporting adverse events (60%, CI95: 50-69), relationships with supervisors (82%, CI95: 73- 88), learning organization and continuous improvement of service (feedback) (59%, CI95: 49-68), teamwork (86%, CI95: 78-91), freedom of expression (67%, CI95: 57-75), not repression of error (49%, CI95: 39-59), human resources (39%, CI95: 30-49), safety management (32%, CI95: 24-42) and teamwork between departments (47%, CI95: 38-57) (Table 3).
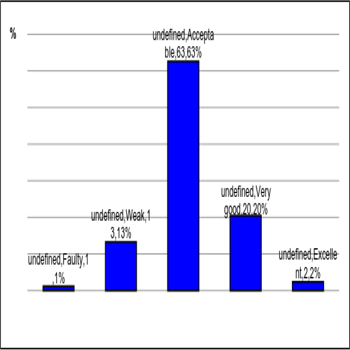
Figure 1: Percentage of responses to the question "Overall, how would you rate the safety of care in your department?"
Differences Observed
There are statistical significant differences between the three sites (Figure 2) for the overall perception of safety (X2 = 22.89, p < 0.001), feedback (X2 = 26.72, p < 0.001), teamwork (X2 = 8.94, p < 0.02) and freedom of expression (X2 = 7.68, p < 0.05). The comparison between jobs showed statistical significant differences (Figure 3) for the frequency of reports (X2 = 25.63, p < 0.001), relationships with supervisors (X2 = 8.31, < 0.05), feedback (X2 = 18.35, p < 0.001) and teamwork (X2 = 9.11, p < 0.05). Comparison according to seniority in the profession showed that persons exercising their profession for more than 5 years had lower scores for all criteria (Figure 4) with statistical differences for overall perception (X2 = 5.09, p < 0.05), feedback (X2 = 14.97, p < 0.001), safety management (X2 = 17.64, p < 0.001 ) and teamwork between departments (X2 = 8.67, p < 0.005).
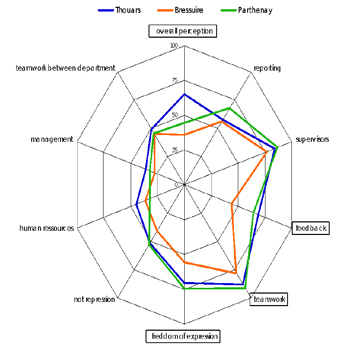
Figure 2: Percentage of positive responses to the ten dimensions of safety culture according to the sites (framed dimensions have statistically significant differences with p < 0.05).
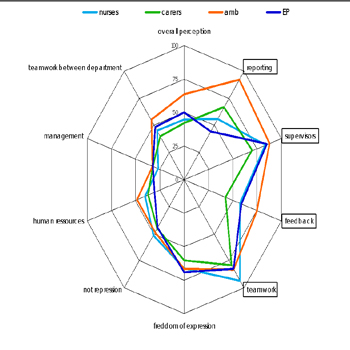
Figure 3: percentage of positive responses to the ten dimensions of safety culture according to the professions (amb: ambulances, EP: emergency physicians, framed dimensions have statistically significant differences with p < 0.05).
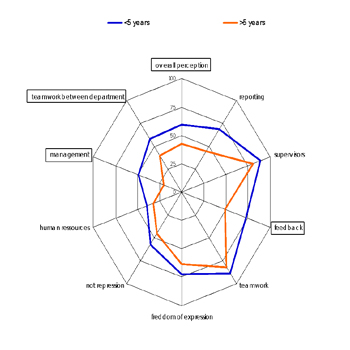
Figure 4: Percentage of positive responses to the ten dimensions of safety culture according to seniority in the profession (framed dimensions have statistically significant differences with p < 0.05).
DISCUSSION
Safety Culture
Safety culture is a concept that has been defined in INSAG-4 1991 report of the Nuclear Energy Agency concerning the analysis of the Chernobyl accident, in which it is shown that improved techniques, procedures, standards and staff training are not enough to improve the security of an organization [13]. If there is consensus on the multidimensional nature of safety culture, there is not on their definition, their number varying from 2 to 19 according to the authors [14]. Past ten years have seen an exponential increase of published works concerning the safety of care [15]. A developed safety culture is related to more near misses intercepted in ED [16]. In the ICU, a safety culture less developed is related to a higher mortality and length of stay [17]. Overall, the promotion of safety culture allows fewer AEs and complications during hospitalization [18].
Global Results
The response rate is very high, superior to those found in the literature [5, 6, 8, 10, 15, 19]. Safety culture of care is generally unsatisfactory with only half of positive responses on the general criterion. A recent international study, with response rates between 52% and 87% showed between 49% and 64% of positive responses on this criterion [6]. 63% [CI: 52-72%] of agents believe that the security level of care is "acceptable" and 20% [CI: 13-30%] "very good" (Figure 1). We found in the literature a rate of 62% acceptable in Dutch hospitals, 43% in Japan, 46% in Taiwan and 22% in hospitals Americans (45% of the respondents felt very good) [6, 8]. Dimensions "reporting errors or adverse events" and "feedback" are related with a positive response rate of respectively 60% and 59%. The dimension "freedom of expression" is penalized by the fact that agents do not feel free to question the decisions of their superiors. Other negative points are the dimensions beyond the perimeter of the ED (non-punitive response, human resources, safety management and teamwork between departments) with the lowest rate of positive responses, less than 50%. These low scores highlight a strategic deficit institution of safety culture of care, with a low level of bureaucratic maturity [20]. The positives scores are excellent for teamwork in the service and the relationships with supervisors (80% of positive responses). This good relationship between agents is an asset for the implementation of corrective measures.
Differences Observed
The differences between sites are due to special events. On the site of Bressuire, emergency physicians are resigned a few years ago and there are difficulties to restore a stable medical team. These difficulties have affected in part "team spirit". On the site of Parthenay, the organization of the short-term hospitalized unit was amended two years ago, against the advice of the direct supervisors and medical team. This non concerted reorganization affected in part the overall perception of security and relationships with the hierarchy. The results are comparable between jobs except in four dimensions. There are more reports of adverse events and more experience feedback by ambulances as other professions. This is probably due to the fact that their work has a large technical part and verification of material with specific procedures. Although statistically significant, differences on the dimensions "teamwork" and "relationships with supervisors" have no practical consequence because they are in all cases with over 70% positive responses.
Perspectives
Culture in an organization is based on the sharing of ideas and values. An analysis of patterns, rules, goals, values and shared data (or not) between the different professions follows logically this survey. Non-punitive response dimension gets only 49% of positive responses, low score found in the international literature, ranging between 17% and 66% depending on the country [6- 8, 21, 22]. The improvement of this dimension would have an impact on the rate of reporting of AEs and errors, on the learning organization and continuous improvement dimension and probably on the freedom of expression dimension. The challenge is to move from the culture of blame errors to the feedback and improving system culture. We are working on a fully anonymous reporting tool of errors or AEs with a shearing system among all. This tool will be an impact on our culture care safety measure.
CONCLUSION
This survey on the safety culture of an ED shows gaps, particularly on the criteria for establishment, but also strong points on which to build from improvement actions. It is part of a process description of ED under cindynic point of view. These results allow the implementation of targeted actions for improvement including the development of a reporting system for AEs and errors with their distribution among all actors.
REFERENCES
- Michel P, Minodier C, Lathelize M, Moty-Monnereau C, et al. (2010). Les evenements indesirables graves associes aux soins observes dans les etablissements de sante. Resultats des enquetes nationales menees en 2009 et 2004, Solidarite Sante (DREES) 2010.
- Health and Safety Executive (HSE). (2005). A review of safety culture and safety climate literature for the development of the safety culture inspection toolkit, Research report 367, 2005, United Kingdom.
- Hospital Survey on Patient Safety Culture. (2010). Agency for Healthcare Research and Quality, Rockville, April 2010.
- Haute Autorite de Sante, La culture de securite des soins: du concept a la pratique, 2010.
- Saturno PJ, Da Silva ZAG, de Oliveira-Sousa SL, Fonseca YA, et al. (2008). Analysis of the patient safety culture in hospitals of the Spanish National Health System, Med. Clin. Barc. 131(3), 18-25.
- Wagner C, Smits M, Sorra J and Huang CC. (2013). Assessing patient safety culture in hospitals across countries. Int. J. Qual. Health Care. 25(3), 213-221.
- Hamdan M and Saleem AA. (2013). Assessment of patient safety culture in Palestinian public hospitals. Int. J. Qual. Health Care. 25(2), 167-175.
- Fujita S, Seto K, Ito S, Wu Y, et al. (2013). The characteristics of patient safety culture in Japan, Taiwan and the United States, BMC. Health. Serv. Res. 13(20).
- Moghri J, Arab M, Saari AA, Nateqi E, et al. (2012). The Psychometric Properties of the Farsi Version of "Hospital Survey on Patient Safety Culture" In Iran's Hospitals, Iran J. Public Health. 41(4), 80-86.
- Vlayen A, Hellings J, Claes N, Peleman H, et al. (2012). A nationwide hospital survey on patient safety culture in Belgian hospitals: setting priorities at the launch of a 5-year patient safety plan, BMJ. Qual. Saf. 21(9), 760-767.
- Occelli P, Quenon JL and Djihoud A. (2010). Measurement of patient care safety culture. Use the measuring tool Guide, May 2010. Evaluation of the Clinical Coordinating Committee and Quality in Aquitaine - CCECQA.
- http://ww3.ac-poitiers.fr/math/prof/resso/cali/ic_ phrek.html
- Murley TE. (1999). Agency for Nuclear Energy, The role of the regulator in promoting and assessing the safety culture, Paris, OECD Publications.
- >Occelli P, Quenon JL, Hubert B, Hoarau H, et al. (2007). The culture of health safety: A rapidly emerging concept, Risk & Quality. 4(4), 207-212.
- Xuanyue M, Yanli N, Hao C, Pengli J, et al. (2013). Literature review regarding patient safety culture. J. Evid. Based Med. 6(1), 43-49.
- Camargo Jr CA, Tsai CL, Sullivan AF, Cleary PD, et al.(2012). Safety climate and medical errors in 62 US emergency departments, Ann. Emerg. Med. 60(5), 555-563.
- Huang DT, Clermont G, Kong L, Weissfeld LA, et al. (2010). Intensive care unit safety culture and outcomes: A US multicenter study, Int. J. Qual. Health Care. 22(3), 151-161.
- Mardon RE, Khanna K, Sorra J, Dyer N, et al. (2010). Exploring relationships between hospital patient safety culture and adverse events. J. Patient Saf. 6(4), 226-232.
- Weaver MD, Wang HE, Fairbanks RJ and Patterson D. (2012). The association between EMS workplace safety culture and safety outcomes, Prehosp. Emerg. Care. 16(1), 43-52.
- Haute Autorite de Sante. (2011). La securite des patients, mettre en oeuvre la gestion des risques associes aux soins en etablissements de sante, Novembre 2011.
- El-Jardali F, Jaafar M, Dimassi H, Jamal D, et al. (2010). The current state of patient safety culture in Lebanese hospitals: A study at baseline, Int. J. Qual. Health Care. 22(5), 386-395.
- Bodur S and E. Filiz. (2010). Validity and reliability of turkish version of "hospital survey on patient safety culture" and perception of patient safety in public hospitals in Turkey, BMC Health Serv. Res. 10(28).