Previous Issues Volume 2, Issue 1 - 2017
Areas of Medico-Legal Unreliability in Personal Injury Cases
Hugh Koch,1*, Paul Elson2
1Chartered Clinical Psychologist and Director, Hugh Koch Associates, Cheltenham, UK and Visiting Professor to School of Law, Stockholm University, Sweden.
2Chartered Clinical Psychologist, Hugh Koch Associates, Cheltenham and Cardiff, UK.
Corresponding Author: Hugh Koch, Chartered Clinical Psychologist and Director, Hugh Koch Associates, Cheltenham, UK, Tel: 0044-1242-263715; E-Mail: [email protected]
Received Date: 17 Dec 2016 Accepted Date: 09 Jan 2017 Published Date: 10 Jan 2017
Copyright © 2017 Koch H
Citation: Koch H and Elson P. (2016). Areas of Medico-Legal Unreliability in Personal Injury Cases. Mathews J Case Rep 2(1): 0024.
ABSTRACT
Personal Injuries following a serious road traffic accident are illustrated. Assessment processes involving initial assessment and reassessment, defendant-instructed assessment and subsequent joint opinion discussions are outlined, giving further support to the progressive and logical medico-legal understanding of trauma and a positive approach to civil litigation.
KEYWORDS
Personal Injury; Medico-Legal Trail; Joint Statements; Medico-Legal Postulates.
INTRODUCTION
Combining clinical and medico-legal analysis of any one particular civil case being litigated is an innovative approach devised by the first author and his colleagues to address both clinical/psychological and medico-legal aspects of complex personal injury cases [1-3]. This unique analysis ensures a comprehensive approach to understanding the key medicolegal processes in psychological assessment. This paper develops this innovative process further and highlights the application of key medico-legal postulates and develops these in respect of dispute resolution and the use of the Joint Statement process, uniquely developed and practiced in the UK (England and Wales).
Background to trauma case Mr. D was a 29 year old man driving alone on a busy arterial road in Cambridge. He was stationary in traffic at an intersection, waiting to turn right. A car approaching from behind collided with the rear of his car at approximately 60 mph. At the time he felt very shocked and although he was afraid he was severely injured, he did not believe he was going to die.
Typical medico-legal trail The comprehensive process adopted by the civil court in the UK is illustrated in figure 1 below:
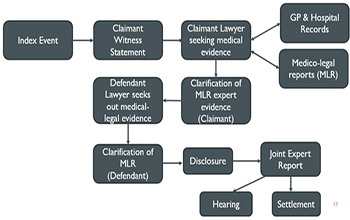
Three aspects of this trail are under scrutiny in this paper: a) Claimant instructed Psychological Assessment b) Reassessment 18 months later c) Joint Statement between claimant-instructed expert and defendantinstructed expert.
Claimant-instructed Psychological Assessment This assessment identified the psychological symptoms of stress, mood disturbance, situational travel anxiety as a driver and passenger, social and work disruption. Diagnosis of a Specific Phobia and multi-factorial Pain Disorder (Physical and Psychological aspects) were made with DSM-IV codes of 300.29 and 307.89 given [4]. At time of assessment, 12 months later, despite some improvement, there were residual symptoms of depressive and recreational drug use to help manage ongoing pain. Psychometric test data was consistent with this. A course of 6 – 8 sessions of CBT was recommended to focus on residual depression and pain coping behaviour. This assessment was consistent with several of Koch's medico-legal postulates, shown in Table 1 below [5]:
Table 1: Relevant Koch Medico-legal Postulates.
| 1. A robust opinion should address diagnosis, causation and attribution, duration and prognosis. 2. A robust opinion will include more than one type of evidence. An opinion based on claimant self-report only may still be valid but is a ‘weak’ opinion in medico legal terms. 3. The classification/diagnostic categories given in DSM 5 and ICD 10 are a part of an expert's opinion/formulation –this systematic check of relevant criteria must be balanced by wider clinic judgement. 4. The expert's Mental State Examination should be consistent with the claimant's description of currently active symptoms – a clear discrepancy reduces the robustness/ strength of an opinion. 5. A robust opinion should include a history of factors which could, on the balance of probabilities, affect a specific index event reaction. 6. A robust opinion should give particular emphasis to the 12 month period prior to and post the index event, but not to the exclusion of earlier or later history. |
Specific identifying details have been removed and the details anonymised in the above case.
Claimant-instructed reassessment
18 months following the first assessment, the claimant had received the recommended CBT therapy and a reassessment was requested by the claimant's solicitors. This identified: • An improvement in some trauma-related psychological symptoms • A worsening of physical pain • Other psychosocial stressors (loss of job; bereavement; family illness and stressors) • Residual trauma related symptoms of low mood, travel anxiety and social and occupational disruption due to ongoing pain. The expert identified characteristics of ‘learned helplessness’ in which the claimant had negative and pessimistic thoughts and feelings about himself which were hampering his improvement and recovery. Further CBT therapy was recommended, with a positive prognosis expected [6]. Joint Statement between claimant-instructed and defendantinstructed experts During this process, and subsequent to the reassessment summarised above, the defendant instructed their own expert to carry out a psychological assessment. This took place approximately 9 months after the claimant-instructed reassessment. This report identified a cluster of symptoms, a duration and prognosis which were largely consistent with the findings of the claimant-instructed expert. In summary, they agreed that as a result of the index car accident: 1. The psychological symptoms attributed to the index accident were stress and trauma, mood disturbance, travel anxiety, social and occupational disruption. 2. The claimant had developed a recognised psychological disorder attributable to the index accident. 3. Although the two experts expressed their diagnoses using slightly different labels/codes, there was significant commonality between the diagnostic labels used. 4. The psychological symptoms were ongoing at the time of the claimant-instructed expert's reassessment and the defendant-instructed expert's assessment 9 months later (which occurred a total of 21 months following the index event). 5. There was no relevant pre-accident distress which impacted on the accident-related problems. This Joint Statement and its relevant discussions between the two experts were carried out in accordance with professional impartiality and logical robustness which were, again, consistent with key medico-legal postulates listed below in (Table 2)
Table 2: Medico-legal Postulates relating to opinion robustness.
| 6. An expert opinion should incrementally increase in robustness over time with access to more data and discussion with other relevant professionals both legal and clinical. 7. An expert's opinion should be the ‘best fit’ professional view of all available data at that time, and should be modified, if appropriate, as and when new data becomes available. 8. It is encumbent on the expert to be impartial, independent of instructing party, and maintain as a high level of logicality as possible when appraising evidence. |
This joint statement process was carried out in line with well established professional guidelines, and reinforced the importance of highlighting causation which was plausible and logical [6, 7].
DISCUSSION AND CONCLUSION
Throughout this case, careful scrutiny was made covering clinical aspects (diagnosis, severity, treatment requirements and likely resolution of symptoms) and medico-legal aspects (causation, multi factorial history, range of opinion, prognosis and material contribution to onset and course of symptoms). The case process was run efficiently by both claimant and defendant teams and the result was that the claimant was recompensed for his injuries, physical and psychological, and the disruption to and time off work. Despite the adversarial process, the use of reassessment, alternative expert assessment and subsequent joint discussion allowed for a professional, logical and comprehensive understanding of the genesis, development and likely resolution of the symptoms and case of Mr. D. In particular, dispute resolution is key to most, if not all, civil cases involving personal injury. The system operating in England and Wales of utilising Joint Statements is unique to the UK and a key characteristic of the ‘therapeutic’ or ‘positive’ approach to understanding and resolving apparent or real differences in opinion in the civil courts.
REFERENCES
- Koch HCH. (2016). Legal Mind: Contemporary Issues in Psychological Injury and Law. Expert Witness Publications. Manchester.
- Koch HCH. (2016). Medico-legal Case Commentary: Interface between Clinical Opinion and Legal Case Reporting in Personal Injury Litigation. Mathews Journal of Case Reports. MJ Case. 1(1): 1-3.
- Koch HCH, Lucas V and Cosway R. (2016). Medico-legal implications of assessing and treating the aftermath of trauma. Scholarena. 3(1).
- APA. (1984). DSM-IV Classification scheme. Washington DC.
- Koch HCH. (2015). Robust opinions need robust reasoning: 15 Medico-legal postulates. Solicitors Journal.
- Koch HCH. (2001). Current medico-legal issues in personal injury litigation. Informa Publications.
- Koch HCH and Elson P. (2016). Plausible causes only, please. Legal Mind Case and Commentary No. 4. Personal Injury Brief Update Law Journal.