Current Issue Volume 10, Issue 2 - 2025
An Adolescent Asymtomatic Case with Uhl Anomaly
Stefan Peters1,*, Axel von Werder2, Jörg Werhahn3
1Medical Care Unit Elze, Cardiology, Germany
2Cardiology, Helios Clinic Hildesheim, Germany
3Radiology, Helios Clinic Hildesheim, Germany
*Corresponding Author: Prof.Dr.med.Stefan Peters, Medical Care Unit Elze, Cardiology, Königsberger Str. 1, 31008 Elze, Germany, Tel: +49 5068 9337022, Email: [email protected]
Received Date: March 11, 2025
Published Date: April 04, 2025
Citation: Peters S, et al. (2025). An Adolescent Asymtomatic Case with Uhl Anomaly. Mathews J Case Rep. 10(2):202.
Copyrights: Peters S, et al. © (2025).
ABSTRACT
Uhl anomaly is a very rare disease. Differential diagnosis are arrhythmogenic right ventricular cardiomyopathy and severe tricuspid regurgitation with right ventricular enlargement. Here we present a 18-year male patient without any complaints. The diagnosis was assessed by echocardiography and cardiac MRI imaging.
Keywords: Uhl Anomaly, Arrhythmogenic Right Ventricular Cardiomyopathy, Paper-Thin Wall, No Right Ventricular Aneurysms.
CASE
An adolescent 18-year old male patient presented in the Medical Care Unit for a certification to play professional handball. Chest pain, exertional dyspnoe, and arrhythmias were denied.
His ECG revealed sinus rhythm, low voltage in limb leads, epsilon wave in V1, and T-wave inversions in inferior leads and in lead V1 to V5/V6 without localized QRS prolongation or terminal activation delay.
Echocardiographic function and appearance to the left ventricle appeared to be normal. The right ventricle was grossly dilated with 50 mm in end-diastolic diameter, paper-thin, and right ventricular aneurysms could be excluded. The right ventricle was severely hypokinetic. The tricuspid valve was slightly insufficient (Figure 1).
.png)
Figure 1. Echocardiography of Uhl anomaly with slight tricuspidal regurgition.
In MRI of the heart these results could be confirmed with no late enhancement of the left ventricle (Figure 2). Massive fibrosis of the right ventricle and hardly myocardium could be proven, right ventricular aneuysms and trabecular structure could be excluded. The diagnosis of asymptomatic Uhl anomaly (right ventricle dysplasia) was made.

Figure 2a. Cardio MRI with gross dilatation of the right ventricle and normal function of left ventricle.
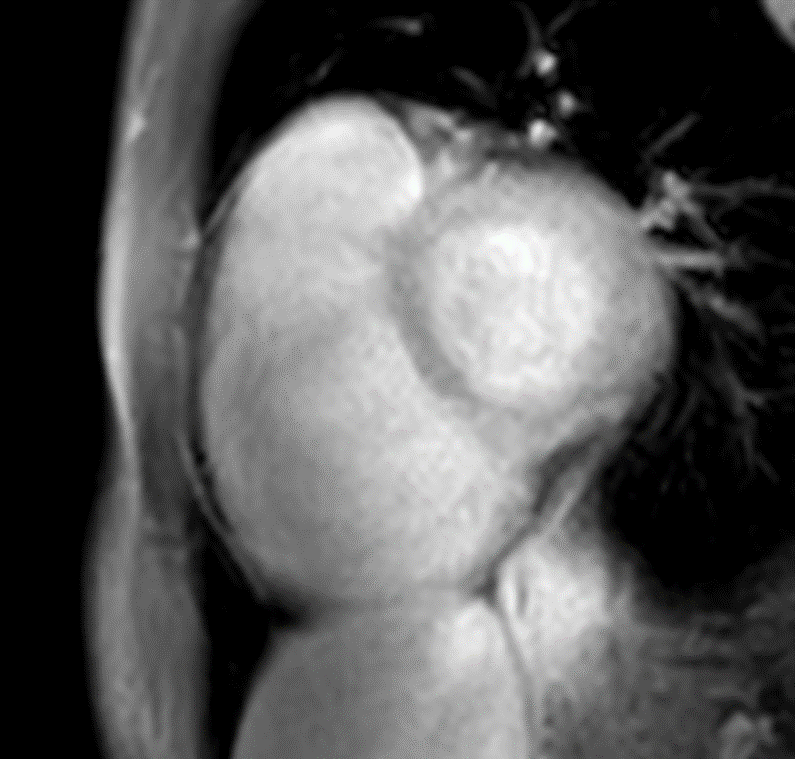
Figure 2b. Cardio MRI with late enhancement of the right ventricle. No late enhancement of the left ventricle.
CONCLUSIONS
The asymptomatic adolescent patient with Uhl anomaly [1] should be observed in a 3 to 6 months follow up. The patient was told not to perform professional handball.
Uhl anomaly is a extremely rare condition, possibly due to interuterine apoptosis of the right ventricle [2]. The dilated right ventricle is hypokinetic, paper-thin, with lacking trabecularisations or aneuryms. Uhl anomaly ends up in progressive heart failure and, to a minor extent, life-threatening arrhythms.
A similar condition is arrhythmogenic cardiomyopathy which includes right ventricular dilatation, right ventricular aneuryms, and highly characteristic ECG changes. Arrhythmogenic cardiomyopathy leads in the majority of cases to arrhythmias and in the minority of cases to heart failure.
The cause of the diseases are completely different with specific gene mutations in arrhythmogenic cardiomyopathy.
In this case of Uhl anomaly the ECG of the patients resembles arrhythmogenic left ventricular or biventricular cardiomyopathy with low voltage im limb leads inferolateral T-wave inversions, but left ventricular function is normal and late enhancement can be excluded.
Epsilon waves can be found in both diseases – arrhythmogenic cardiomyopathy and Uhl anomaly, but also in coronary artery disease [3] and in cardiac sarcoidosis [4]. The ECG in Uhl anomaly is not presented in many case reports, seems to be unspecific.
In this case report extensive T-wave inversions anterolateral are a hint of right ventricular dilatation related to arrhythmogenic cardiomyopathy [5], and possibly plays a role in risk assessment of sudden arrhythmic death.
Another option is right ventricular sarcoidosis. Typical ECG findings are: right precordial T-wave inversions, low voltage in limb leads, epsilon waves, atrioventricular conduction abnormalities, and precordial R‘ waves [6]. The ECG of the patient reveals three positive criteria, atrioventricular conduction abnormalities and significant precordial R‘ waves are missing. In cardiac MRI, however, there is no hint of right ventricular sarcoidosis.
Nevertheless, the ECG of the patient suggests that Uhl anomaly seems to be the maximum variant of arrhythmogenic right ventricular cardiomyopathy, although differences (no fatty infiltration, no right ventricular aneurysms or trabecular structure) exist.
ACKNOWLEDGMENTS
None.
CONFLICTS OF INTEREST
The auhtors declere that there is no conflicts of interest.
REFERENCES
- UHL HS. (1952). A previously undescribed congenital malformation of the heart: almost total absence of the myocardium of the right ventricle. Bull Johns Hopkins Hosp. Sep;91(3):197-209.
- James TN. (1997). Apoptosis in congenital heart disease. Coron Artery Dis. 8(10):599-616.
- Kaiser GA, Waldo AL, Harris PD, Bowman FO Jr, Hoffman BF, Malm JR. (1969). New method to delineate myocardial damage at surgery. Circulation. (5 Suppl 1):I83-I89.
- Omotoye S, Junpaparp P, McHugh J, Silva J, Kuk R, Sackett M, et al. (2021). Cardiac Sarcoidosis With Prominent Epsilon Waves: A Perfect Phenocopy of ARVC. JACC Case Rep. 3(8):1097-1102.
- Peters S. (2014). Electrocardiographic criteria and outcome in patients with arrhythmogenic right ventricular cardiomyopathy. Re: Electrocardiographic predictors of electroanatomic scar size in arrhythmogenic right ventricular cardiomyopathy: implications for arrhythmic risk stratification. Int J Cardiol. 174(3):723.
- Hoogendoorn JC, Venlet J, Out YNJ, Man S, Kumar S, Sramko M, et al. (2021). The precordial R' wave: A novel discriminator between cardiac sarcoidosis and arrhythmogenic right ventricular cardiomyopathy in patients presenting with ventricular tachycardia. Heart Rhythm. 18(9):1539-1547.