Previous Issues Volume 1, Issue 1 - 2016
A Comprasion of Our Mid-level Learning Curve Laparoscopic Appendectomies Experience with Open Appendectomies
Cesim Irsi
1Department of Pediatric Surgery, Istanbul Fatih Sultan Mehmet Teaching and Research Hospital, Atasehir, Istanbul, Turkey.
Corresponding Author:Cesim Irsi, Department of Pediatric Surgery, Istanbul Fatih Sultan Mehmet Teaching and Research Hospital, Atasehir, Istanbul, Turkey, Tel: + 90 532 2262072; E-Mail: [email protected]
Received Date: 25 May 2016 Accepted Date: 21 Jul 2016 Published Date: 11 Aug 2016
Copyright © 2016 Irsi C
Citation: Irsi C. (2016). A Comprasion of Our Mid-level Learning Curve Laparoscopic Appendectomies Experience with Open Appendectomies. Mathews J Pediatr. 1(1): 002.
Aim: We aim to compare our preliminary laparoscopic appendectomy experience with open ones as a clinic which at the mid-level of learning curve for laparoscopic appendectomies.
Material and Methods: Clinic files of children operated due to acute appendicitis were retrospectively analyzed as two groups; laparoscopic appendectomy and open appendectomy. Data including age, sex, operative time, postoperative feeding time, length of hospitalization, complications and comorbidities were analyzed.
Results: At our hospital by the same surgeon, 51 children were operated with the diagnosis of appendicitis during May 2013 to June 2014. These appendectomies were done as open appendectomies in 36 and laparoscopic appendectomies in 15 children. The patients were 22 girls and 29 boys. The average age for open appendectomies were 12.5 ± 5.2 and for laparoscopic appendectomies were 13.9 ± 4.1. Laparoscopic appendectomies were successfully performed on 15 except one due to mechanical problem. Mean operative time was 45 ± 15 minutes, and 55 ± 15m for the OA and LA groups respectively (p > 0.05). Postoperative oral intake time was 24h ± 6h with no difference in both groups. The duration of hospitalization was 2 ± 0.5 days for OA and 1.5 days ± 0.5 for LA with no obvious difference (p > 0.05). Comorbidities found during OA were a hyperplastic polyp at ileal intestinal segment which was successfully removed and for LA group; a paraovarian cyst and a liver hemangiomas were detected (p < 0.05). Main complications for OA were 3 wound infections and an intestinal adhesive lesion which resolved spontaneously with clinical follow up and one trocar side skin infection occurred in LA group which was treated properly.
Conclusion: As a new clinic which is at the mid-level of laparoscopic appendectomy learning curve we found no certain differences between open and laparoscopic appendectomies regarding operative time, postoperative initiation of oral intake time and duration of hospitalization. Laparoscopic appendectomies provide less postoperative pain, better adaptation to daily activities, better cosmetic results and beside all these due to availability of intra-abdominal visual exposure we can determine possible comorbidities without further surgical operations.
Appendectomy; Laparoscopic Appendectomy; Learning Curve; Comorbidity; Children.
INTRODUCTION
Acute appendicitis is one of the most common surgical procedures performed by pediatric surgeons [1, 2]. Recently minimal invasive surgery take a great popularity among pediatric surgeon primarily due to its surgical field exposure and postoperative conformity superiority over to the conventional treatment. Despite its popularity and advantage, laparoscopic surgery includes some struggle like equipment and appropriate skill to successfully perform appendectomy procedures. According to a previous papers despite its general acceptance all over the world, laparoscopic appendectomies are performed frequently only by 31 % of pediatric surgeons and 39% of them do rarely [3, 4]. This fact is mostly due to technical equipment availabilities difficulties and lack of surgeon familiarity with the procedure. That is why we perform this study to share our preliminary laparoscopic appendectomy experience with open ones according to advantage and disadvantage as a new clinic which is at the midlevel of learning curve of laparoscopic appendectomies.
METHODS
The files of 51 patients whose were diagnosed as appendicitis and operated via open (OA) or laparoscopic appendectomies (LA) were reviewed from May 2013 to June 2014. The consent of the patients for operations were taken from all of the families. The all operations were performed by the same pediatric surgeon. The patients were divided into two groups as open appendectomy and laparoscopic appendectomy (Table 1). The complicated appendicitis (perforated and gangrenous) were performed as open surgery (Figure1).
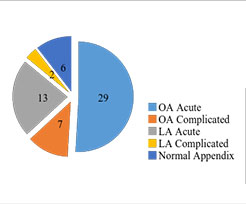
Figure 1: Study population of appendicities* *Postoperative diagnosis, according to the pathology reports.
Table 1: The preoperative patients demographics (N:51)*.
| Open Appendectomies (n:36 ) | Laparoscopic Appendectomies (n:15) | |
|---|---|---|
| Mean age (y) | 12.5 ± 5.2 | 13.9 ± 4.1 |
| Gender (male/female) | 18/18 | 11/4 |
| Acute Appendicitis | 29 | 13 |
| Complicated Appendicitis | 7 | 2 |
*6 patients with normal appendicitis as reported postoperatively were not excluded.
The results of both groups were compered according to age, sex, operative time, postoperative oral intake, duration of hospitalization, comorbidities and complications (Table 2). Laparoscopic appendectomies were performed by three ports as intracorporal after establishment of pneumo peritoneum by a verses needle (10mm trocar from umbilicus, 5mm one from left lover quadrant and another 5mm one from right upper quadrant of abdomen), mesentery of appendix were dissected by ligature and appendicitis mobilization in case of need by a hook cautery. Appendicitis were double ligated at the stump via 2/0 prolen endo loop suture and then appendix were excised by ligature. The appendicitis specimens were mostly taken out of the abdominal cavity by an endobag or directly through a trocar opening. The procedures were terminated after irrigation and aspiration of abdominal cavity especially for cases which contaminated or presence of intra-abdominal exudate.
Table 2: The comparison of postoperative variables of open (OA) and laparoscopic (LA) appendectomies.
| Open Appendectomies | Laparoscopic Appendectomies | p value | |
|---|---|---|---|
| Mean operative time(minute) | 45 ± 15 | 55 ± 15 | p > 0.05 |
| Postoperative oral Intake time(hour) | 24 ± 4 | 18 ± 4 | p > 0.05 |
| Hospitalization time (hours) | 48 ± 12 | 36 ± 12 | p > 0.05 |
| Comorbidities* | 1 | 3 | p < 0.05 |
| Complication ** | 4 | 1 | p > 0.05 |
*Low sample size was a burden (n:51 and 15 laparoscopic appendectomies). **3 wound infection and 1 adhesive intestinal disease in OA group and 1 trocar side skin infection (endobag not used) in LA group.
Open appendectomies were performed with right lower quadrant transverse muscle- splitting abdominal incisions and after mesentery dissection by monopolar cautery, double ligation of appendicitis at its base and then with excision of appendix, appendectomy were concluded. The stump of appendicitis were mostly buried to cecum serosa via persisting suture in open ones. We didnt use drain placement at any type of the appendectomies cases. The all appendectomy specimens were send to pathology department and classification were performed as simple, perforated and gangrenous according to the pathology reports (Figure 1). Statistical evaluation were performed by using chi-squared P values and a statistical significance was established as P < 0.05.
RESULTS
At our clinic; 51 appendectomies (36 open appendectomies and 15 laparoscopic appendectomies) were performed in children with a preoperative diagnosis of appendicitis by the same pediatric surgeon. The patients were girls in 22 cases and boys in 29 cases. The average age of open appendectomies (OA) was 12.5 ± 5.2 and for laparoscopic appendectomies were 13.9 ± 4.1. There was no significant statistical differences between both groups regarding with average patients age (P > 0.05). We determined operation types according to whether proper equipment existence and patients diagnosis were an acute or a complicated appendicitis. Complicated appendicitis were performed as open surgery. Laparoscopic appendectomies were performed in 15 patient except one due to the mechanical problem and then open appendectomy were performed successfully. Both appendectomy groups (OA, LA) were compared regarding with mean operation time, postoperative oral intake time and mean postoperative hospitalization time. There were no any statistical significance were found regarding between these postoperative variables (P > 0.05). Mean operation time which is defined as starting time of skin incision until to last surgical suture ligation time, for OA group was 45 ± 15minutes and for LA group was 55 ± 15 minutes. The mean postoperative oral intake time was 24 ± 4 for OA and 18 ± 4hr for LA groups without any statistical significance. The mean postoperative hospitalization time until discharge were 2 ± 0.5 day for OA and 1.5 ± 0.5 day for LA groups without any statistical significance (P > 0.05), (Table 2). Total mean hospital charges were $ 200 for open appendectomies (OA) and $ 300 for laparoscopic appendectomies (LA). There were 3 comorbidities; diagnosed intraoperatively among those 51 appendectomies patients; 1 an ileal intestinal segment hyperplastic polip (2.9 %) for OA and 2 comorbidities detected during laparoscopic appendectomies as a paraovarian cyst and a hepatic haemangioma-hamartom (13.3 %), (P < 0.05), (Table 2). As a complication in OA group we observed 3 wound infections and an intestinal adhesive lesion which resolved spontaneously during clinical follow up and a trocar side skin infection in LA group which was treated by antibiotherapy properly. There was no any mortality in both appendectomy groups (Table 2).
DISCUSSION
Laparoscopy at the age of minimal invasive surgery beside magnified image and direct exposure of surgical field enable us exposure of other intra-abdominal structure like pelvic organelles and part of the upper gastro-intestinal systems. That is why it is very appropriate to perform appendectomy (which is the most common pediatric emergency) laparoscopically [1, 2]. Open appendectomy cannot provide us intra-abdominal exposure without large skin incision. At the decision make up step for selection types of the appendectomy procedure, we mostly checked availability of all proper equipment existence for laparoscopic surgery and patient definite diagnosis as acute or complicated, although recent study reveal laparoscopy for even complicated appendicitis can be performed successfully [5-7]. Learning curve was defined as approximately 20 laparoscopic appendectomies in 5 year period in the english speaking literature [8-10]. As a clinic at the mid-level of learning curve; our postoperative results like operative time and postoperative oral intake time were mostly determined by our pneumoperitoneum establishment time via verses needle and trocar replacement times and manipulation to isolate appendicitis from ileum, cecum and other surrounding tissues like peritoneum and omentum. Because less muscle dissection leads less post-operative pain and less cecal-ileac manipulation time means low risk of intestinal peristaltic blockage occurrence means rapid recovery for initiation for oral intake, less hospitalization time and early discharge from hospital [7, 11-13]. We mostly ordered to oral intake after postoperative 1th day in both group and this time directly affected by intestinal manipulation degree to prepare appendix and trocar replacement time. After oral intake both open and laparoscopic appendectomies patients were discharged on their postoperative 1th-2th day without any problem. There was no any statistical significance (P > 0.05) between these both post operative variables. Early postoperative oral intake has been widely accepted recently between pediatric surgeons and this tendency leads early discharge rate from hospital beside relatively low cost of it [12, 13]. One paraovarian cyst < 3cm and a hepatic haemangioma were detected during intra-abdominal exposure at laparoscopic appendectomies groups. Although our sample size was small, it is well known that laparoscopic appendectomy with direct visualization property has superiority to open ones [13-15]. In open ones only careful palpation may help identification of comorbidities. We found an ileac intestinal segment hyperplastic pulp as a comorbidities among 36 open appendectomies via careful palpation and inspection in operatively. A few complications were detected among those appendectomies and these were a trocar side skin infection in laparoscopic group which was developed because of direct extraction of the appendicitis specimen through trocar opening and in open appendectomies group as a complications; we observed 3 wound infections and an intestinal adhesive lesion in a complicated case which resolved spontaneously during clinical follow up. The trocar side skin infection can be prevented by routine usage of endobag. So by this way we can prevent spillage and contamination of intra-abdominal organelles and trocar skin side by highly infectious appendicitis [7, 13, 16, 17]. Intestinal adhesive lesions are well known postoperative complication of any open intra-abdominal surgery but in our small sample size and as other reported papers no any direct correlation between laparoscopic appendectomy and increased adhesive lesions occurrence rate [18-23]. Although our relatively small sample size is a burden for us to reach an obvious conclusion about a well-known pediatric surgery topics but knowledge of low laparoscopic usage ratio all over the world among pediatric surgery clinics as we mentioned above encourage us to share our preliminary laparoscopic experience.
CONCLUSION
Laparoscopic appendectomies can be performed as successfully as open appendectomies in pediatric patients as our preliminary study demonstrate and seemed to show obvious advantages compared to open appendectomies like the results of the same literature studies.
REFERENCES
- Browses introduction to the symptoms and signs of surgical disease 4 edition. (2005). Hodder Arnolc.
- Addiss DG, Shaffer N, Fowler S and Tauxe RV. (1990). The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 132(5), 910-925.
- Newman K, Ponsky T, Kittle K, Dyk L, et al. (2003). Appendicitis 2000: variability in practice, outcomes, and resource utilization at thirtypediatric hospitals. J Pediatr Surg. 38(3), 372-379.
- Muehlstedt SG, Pham TQ and Schmeling DJ. (2004). The management of pediatric appendicitis: a survey of North American pediatric surgeons. J Pediatr Surg. 39(6), 875-879.
- Wei B, Qi CL, Chen TF, Zheng ZH, et al. (2011). Laparoscopic versus open appendectomy for acute appendicitis: a metaanalysis. Surg Endosc. 25(4), 1199-1208.
- Wang X, Zhang W, Yang X, Shao J, et al. (2009). Complicated appendicitis in children: is laparoscopic appendectomy appropriate? A comparative study with open appendectomy - our experience. J Pediatr Surg. 44(10), 1924-1927.
- Yagmurlu A, Vernon A, Barnhart DC, Georgeson KE, et al. (2006). Laparoscpic appendectomy for perforated appendicitis: a comparison with open appendectomy. Surg Endosc. 20(7), 1051-1054.
- Canty TG Sr, Collins D, Losasso B, Lynch F, et al. (2000). Laparoscopic appendectomy for simple and perforated appendicitis in children: the procedure of choice? J Pediatr Surg. 35(11), 1582-1585.
- Foulds KA, Beasley SW and Maoate K. (2000). The effect of the availability of laparoscopic techniques on the treatment of appendicitis in children. Pediatr Surg Int. 16(7), 490-492.
- Dagash H, Chowdhury M and Pierro A. (2003). When can I be proficientin laparoscopic surgery? A systematic review of the evidence. J Pediatr Surg. 38(5), 720-724.
- Esposito C, Borzi P, Valla JS, Mekki M, et al. (2007). Laparoscopic versus Open Appendectomy in Children: A retrospective comparative study of 2,332 cases. World J Surg. 31(4), 750-755.
- Lee SL, Yaghoubian A and Kaji A. (2011). Laparoscopic vs Open Appendectomy in Children: Outcomes Comparison based on Age, Sex, and Perforation Status. Arch Surg. 146(10), 1118-1121.
- Fleming FJ, Kim MJ, Messing S, Gunzler D, et al. (2010). Balancing the risk of postoperative surgical infections: a multivariate analysis of factors associated with laparoscopic appendectomy from the NSQIP database. Ann Surg. 252(6), 895-900.
- Oka T, Kurkchubasche AG, Bussey JG, Wesselhoeft CW, et al. (2004). Open and laparoscopic appendectomy are equally safe and acceptable in children. Surg Endosc. 18(2), 242-245.
- Vegunta RK, Ali A, Wallace LJ, Switzer DM, et al. (2004). Laparoscopic appendectomy in children: technically feasible and safe in all stages of acute appendicitis. Am Surg. 70(3), 198-202.
- Nataraja RM, Bandi A, Clarke SA and Haddad MJ. (2010). Comparison of intra-abdominal abscess formation following laparoscopic and open appendicectomy in children. J Laparoendosc Adv Surg Tech A. 20(4), 391-394.
- Romy S, Eisenring MC, Bettschart V, Petignat C, et al. (2008). Laparoscope using and surgical site infections in digestive surgery. Ann Surg. 247(4), 627-632.
- Rosin D, Zmora O, Hoffman A, Khaikin M, et al. (2007). Low incidence of adhesion-related bowel obstruction after laparoscopic colorectal surgery. J Laparoendosc Adv Surg Tech A. 17(5), 604-607.
- Andersson RE. (2001). Small bowel obstruction after appendicectomy. Br J Surg. 88(10), 1387-1391.
- Leung TT, Dixon E, Gill M, Mador BD, et al. (2009). Bowel obstruction following appendectomy: what is the true incidence? Ann Surg. 250(1), 51-53.
- Krisher SL, Browne A, Dibbins A, Tkacz N, et al. (2001). Intra-abdominal abscess after laparoscopic appendectomy for perforated appendicitis. Arch Surg. 136(4), 438-441.
- Paik PS, Towson JA, Anthone GJ, Ortega AE, et al. (1997). Intraabdominal abscesses following laparoscopic and open appendectomies. J Gastrointest Surg. 1(2), 188-192.
- Katkhouda N, Friedlander MH, Grant SW, Achanta KK, et al. (2000). Intraabdominal abscess rate after laparoscopic appendectomy. Am J Surg. 180(6), 456-459.