Previous Issues Volume 2, Issue 1 - 2017
Evolution of Subtypes of the Human Immunodeficiency Virus Type 1 in Kinshasa over the Last 30 years: Documentary Review from 1985 to 2015
Erick Ntambwe Kamangu1, 2*, Berry Bongenia Ikolango2, Ben Bulanda Ilunga2
1Molecular Biology Service, Department of Basic Sciences, Faculty of Medicine, University of Kinshasa, Kinshasa-Democratic Republic of Congo.
2Research Group, Focus HIV/AIDS, Kinshasa-Democratic Republic of Congo.
Corresponding Author: Erick N. Kamangu, Molecular Biology Service, Department of Basic Sciences, Faculty of Medicine, University of Kinshasa, Kinshasa-Democratic Republic of Congo, Tel: +243 (0) 81 54 01; E-Mail: [email protected]
Received Date: 07 Feb 2017 Accepted Date: 14 Feb 2017 Published Date: 20 Feb 2017
Citation: Kamangu EN, Ikolango BB, and Ilunga BB. (2017). Evolution of Subtypes of the Human Immunodeficiency Virus Type 1 in Kinshasa over the Last 30 years: Documentary Review from 1985 to 2015. Mathews J HIV AIDS. 2(1): 014.
ABSTRACT
Context: More than 30 years after its official declaration, the infection by HIV is still a major public health problem in Kinshasa. This HIV epidemic is dominated by the group M of Type 1, which is subdivided into several subtypes and CRF. Objective: The objective of this review was to expose the specificities of the HIV-1 epidemic in Kinshasa, in terms of the evolution of different variants of HIV over time. Methodology: A literature review was carried out on various publication and abstract papers presented on conference focusing on the identification of the different variants of HIV Type 1 in Kinshasa, DRC. This research was limited to the published works and abstracts presented over the past 30 years. Results: According to the different documentary sources, the subtype A of group M of HIV Type 1 remained more or less majority over time in Kinshasa. In 1985, subtype G was predominant at 37.5% followed by subtypes a (20.8%). In 1997, subtype A was the majority with 43.7% followed by subtypes D (13.4%). In 2000, subtype A was dominant at 42.2% followed by subtypes G (25.3%). In 2002, subtype A was predominant at 39.6% followed by subtype D (13.9%). In 2007, subtype A was in the majority at 23.0% followed by subtypes C (13.8%). By 2015, subtype A was also dominant with 22.9% followed by the CRF02_AG (11.1%). Conclusion: The HIV-1 molecular epidemic in Kinshasa suggests persistence of subtype A and a significant increase in CRF02_AG in the general population over time.
KEYWORDS
Evolution; HIV-1 Subtypes; Epidemiology; Kinshasa.
INTRODUCTION
More than 30 years after its official declaration, the infection by the Human Immunodeficiency Virus (HIV) remains a major public health problem in Kinshasa and even for the entire Democratic Republic of Congo (DRC). The prevalence of the HIV epidemic in Kinshasa was of 1.6% according to the reports of the Demographic Health Survey (DHS) in 2014 [1]. It has remained more or less stable below 5% since the beginning of this century for the country. HIV, which is a Lentivirus of the Retroviridae family, has a diversity that is equal to the complexity of its treatment. This virus is divided into 2 types (HIV-1 and HIV-2), each of which is divided into different groups, subtypes and recombinant forms [2]. In the DRC, in Kinshasa in particular, the HIV epidemic is dominated by the group M of Type 1 [3]. This group M comprises several subtypes and Circulating Recombinant Forms (CRFs) as well as Unknown Recombinant Forms (URFs) which stayed very dynamically in Kinshasa. Since 1985, with the first phylogenetic study on the population of Kinshasa, the distribution of strains circulating in the city has changed considerably; it is in constant evolution. Some subtypes have been confirmed over time while others gradually disappear due to pressure and different selections [4]. The objective of this review was to expose the specificities of the HIV epidemic in Kinshasa, in terms of the evolution of different variants of HIV over time.
METHODOLOGY
Literature ReviewVarious publications and abstract papers presented at a conference focusing on the identification of the different variants of HIV Type 1 in Kinshasa, in the Democratic Republic of Congo (DRC), were the subject of this review. The search for these published works on the various variants of HIV Type 1 was done on the internet from the following websites: (i) MEDLINE / PubMed; (ii) POPLINE electronic database of published documents; (iii) Public access data on conference papers; (iv) Scientific report published on the Internet; (v) Google Scholar; (vi) Cochrane Library. This online research was based on the following keywords: “HIV, subtype, Kinshasa”, “genotype, HIV, Kinshasa” and “HIV strains in Kinshasa”.
Inclusion and non-inclusion criteria The research was restricted to published works and abstracts presented over the last 30 years (1985 to 2015). The manuscripts were selected according to the relevance of the methodology, the results as well as the representativeness of the samples. The socio-demographic information of the studied population, the measurement methods, and the objectives were considered in the evaluation of the articles. Reading the various articles made it possible to exclude articles that did not directly concern the HIV-1 strains circulating in Kinshasa. Pediatric studies, studies on migrant populations as well as studies without original data were not retained for this review.
RESULTS
According to the various documented sources, published articles and abstracts presented in the conference since 1985, the subtype A of group M of HIV Type 1 remained more or less majority over time for Kinshasa. In 1985, subtype G was predominant at 37.5%, followed by subtypes A (20.8%), F (12.5%), U (12.5%) and CRF01_AE (8.3 %) [4]. In 1997, subtype A was predominant with 43.7% followed by subtypes D (13.4%), G (10.5%), H (9.8%) and U (7.7 %) [5, 6]. In 2000, subtype A was dominant at 42.2% followed by subtypes G (25.3%), D (10.8%), C (6.0%) and F (4, 8%) [7]. In 2002, subtype A was predominant at 39.6% followed by subtypes D (13.9%), G (10.4%), C (9.7%) and U (7.6%) [8]. In 2007, subtype A was predominant at 23.0% followed by subtypes C (13.8%), G (5.3%), D (4.3%) and U (2.1%) [9]. By 2015, subtype A was also dominant with 22.9% followed by CRF02_AG (11.1%), subtypes C (9.8%), G (9.8%) and K (9.8% %) [10]. Table 1 presents the different subtypes according to the years. Figure 1 shows the evolution of strains over the years.
Table 1: Evolution of subtypes of the Human Immunodeficiency Virus Type 1 in Kinshasa over the last 30 years (1985-2015).
| Subtypes of groupe M | 1985 (n=24) | 1997 (n=142) | 1999-2000 (n=83) | 2002 (n=144) | 2007 (n=94) | 2015 (n=153) |
|---|---|---|---|---|---|---|
| A | 5 (20.8%) | 62 (43.7%) | 35 (42.2%) | 57 (39.6%) | 22 (23.0%) | 35 (22.9%) |
| B | 0 | 0 | 0 | 0 | 0 | 3 (2%) |
| C | 0 | 3 (2.2%) | 5 (6.0%) | 14 (9.7%) | 13 (13.8%) | 15 (9.8%) |
| D | 1 (4.2%) | 19 (13.4%) | 9 (10.8%) | 20 (13.9%) | 4 (4.3%) | 12 (7.8%) |
| E | 0 | 1 (0.7%) | 0 | 0 | 0 | 0 |
| F | 3 (12.5%) | 8 (5.6%) | 4 (4.8%) | 2 (1.4%) | 0 | 6 (3.9%) |
| G | 9 (37.5%) | 15 (10.5%) | 21 (25.3%) | 15 (10.4%) | 5 (5.3%) | 15 (9.8%) |
| H | 1 (4.2%) | 14 (9.8%) | 3 (3.6%) | 9 (6.3%) | 1 (1.1%) | 12 (7.8%) |
| J | 0 | 5 (3.5%) | 2 (2.4%) | 2 (1.4%) | 1 (1.1%) | 9 (5.9%) |
| K | 0 | 4 (2.8%) | 1 (1.2%) | 4 (2.8%) | 0 | 15 (9.8%) |
| CRF01_AE | 2 (12.5%) | 0 | 0 | 4 (2.8%) | § | 5 (3.3%) |
| CRF02_AG | 0 | 0 | 0 | 3 (2.1%) | § | 17 (11.1%) |
| CRF05_DF | 0 | 0 | 0 | 2 (1.4%)§ | 0 | |
| CRF11_cpx | 0 | 0 | 0 | 1 (0.7%)§ | 0 | |
| U | 3 (12.5%) | 11 (7.7%) | 3 (3.6%) | 11 (7.6%) | 2 (2.1%) | 8 (5.2%) |
§Prevalence of individual CRF not defined in this study (14 CRFs and 32 URFs).
DISCUSSION
The objective of this review was to expose the specificities of the HIV epidemic in Kinshasa, in terms of the evolution of different variants of HIV over time. Six (6) published works have been documented particularly for Kinshasa from 1985 to 2015 with the main objective of determining the strains of the HIV Type 1 circulating in Kinshasa. In 1985, Yang et al worked on 24 positive HIV samples harvested by the AIDS Project exclusively on Professional Sex Workers (PSW) from Kinshasa [4]. This female-only population had an average age of 22.2 ± 4.6 years [11]. Subtype G was predominant at 37.5%, followed by subtypes A (20.8%), F (12.5%), U (12.5%), CRF01_AE (8.3%), subtypes D (4.2%) and H (4.2%) [4]. A more recent study of a PSW population was published in 2016 with subtypes presented as follow: subtype K was dominant with 25% followed by subtypes A (15%), G (15%), C (10%), J (10%), U (10%), CRF02_AG (10%) and subtype H (5%) [12]. These works demonstrate that PSWs, because of the diversity of their partners, present molecular epidemiology different from that of the general population and that this population should not be neglected when planning for HIV subtypes surveillance.
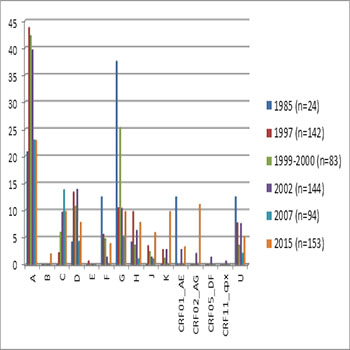
Figure 1: Subtypes of HIV Type 1 in Kinshasa throughout the past 30 years.
In 1997, Mulanga-Kabeya C et al worked on a population of 142 young HIV positive adults aged 20-30 years, including 50 tuberculosis patients, 26 clinic patients, 16 women included from the Prenatal Consultation programs, 10 blood donors, 29 PSWs and 12 patients of diverse origin [5]. The mean age of the population was 25.2 ± 6.3 years [5]. Subtype A was predominant with 43.7%, followed by subtypes D (13.4%), G (10.5%), H (9.8%), U (7.7%), F (5.6%), J (3.5%), K (2.8%), C (2.2%) and E (0.7%) [5, 6]. In 1999-2000, Yang C et al worked on 83 positive HIV samples, of which 42 were from PSs, 29 from clinic patients and 12 from tuberculosis patients [7]. Patients were included in the 18-49 years range of age [7]. Subtype A was dominant at 42.2% followed by subtypes G (25.3%), D (10.8%), C (6.0%), F (4.8%), H (3.6%), U (3.6%), J (2.4%) and K (1.2%) [7]. In 2002, Vidal N et al worked on a heterogeneous population of 144 HIV-positive patients, including 49 tuberculosis patients, 39 clinic patients, 3 women included from the Prenatal Consultation programs, 37 PSWs and 16 patients of diverse origin [8]. The mean age of the patients was 29.4 ± 9.6 years [8]. Subtype A was predominant at 39.6% followed by subtypes D (13.9%), G (10.4%), C (9.7%), U (7.6%), H (6.3%), K (2.8%), CRF01_AE (2.8%), CRF02_AG (2.1%), F (1.4%), J (1.4%), CRF05_DF (1 , 4%) and CRF11_cpx (0.7%) [8]. In 2007, Djoko CF et al have worked on HIV positive samples from 94 soldiers, 92.5% of men and 7.5% of women [9]. The median age of the population was 35 years with limits of 20 and 63 years [9]. The subtype A had a majority at 23.0% followed subtype C (13.8%), G (5.3%), D (4.3%), U (2.1%), H (1.1%) and J (1.1%) [9]. Of the 94 samples, 14 (14.9%) were CRFs (CRF01_AE, CRF02_AG, CRF11_cpx, CRF13_cpx, CRF25_ cpx, CRF26_A5U, CRF37_cpx, CRF43_02G and CRF45_cpx) and 32 (34.0%) were URFs [9]. In 2015, Kamangu NE et al have worked on a heterogeneous population of 153 HIV patients including 92 women and 61 men all aged over 18 years through the 4 districts of Kinshasa [10]. The median age of this population was 37 years with limits of 18 and 65 years [10]. These 153 patients were newly infected patient eligible to Antiretroviral Treatment and ART-naive followed in different centers of the city [10, 13]. Eight (8) Ambulatory Treatment Centers (ATC), in order of 2 ATCs per district, participated in this study. All social strata have been represented in this study [10]. These ATCs were selected because of the reproducibility criteria [14]. In this population, the subtype A was predominant with 22.9% followed CRF02_AG (11.1%), subtypes C (9.8%), G (9.8%), K (9.8 %), D (7.8%), J (5.9%), U (5.2%), F (3.9%), CRF01_AE (3.3%) and subtype B (2%) [10]. Subtype A of HIV Type 1 M is continuously the present strain of high prevalence in Kinshasa since the epidemic was declared in 1983. Since the first phylogenetic studies with the population of Kinshasa in 1985, this strain was present with a high prevalence and it has been maintained throughout the years [4-10]. Although still a majority, subtype A has lost points in recent years: from 43.7% in 1997 to 22.9% in 2015 [5, 6, 10]. This dominant prevalence may be due to the intragroup diversity of subtype A, which is divided into 4 subtypes (A1, A2, A3, and A4), which makes it more apt to escape conventional treatments [15]. Subtype B, which was not present in the city in previous years, is now counted among the strains circulating in Kinshasa [10]. This is a case of importation of HIV infection from northern countries where this subtype occurs to the south. Hence the movement of populations is always a factor that influences the global epidemic, the distribution, and evolution of the different strains of the HIV virus. Subtypes C, D, F, G, H, U, and CRF01_AE have lost scope in the epidemic in Kinshasa throughout the years in the city (Figure 1). Subtype C decreased from 13.8% in 2007 to 9.8% in 2015 [9, 10]. Subtype D decreased from 13.9% in 2002 to 7.8% in 2015 [8, 10]. Subtype F decreased from 12.5% in 1985 to 3.9% in 2015 [4, 10]. Subtype G decreased from 37.5% in 1985, to 25.3% in 2000 to 9.8% in 2015 [4, 7, 10]. Subtype H decreased from 9.8% in 1997 to 7.8% in 2015 [5, 6, 10]. The subtype U decreased from 12.5% in 1985, 7.6% in 2002 to 5.2% in 2015 [4, 8, 10]. The CRF01_AE decreased from 12.5% in 1985 to 3.3% in 2015 [4, 10]. Phylogenetic analyses using the Neighbors-joining and maximum likeness approach demonstrated that the abovementioned strains were quite similar to subtype B; hence their difficulty in escaping conventional treatments [16]. On the other hand, subtypes J and K have become more present in the epidemic than in previous years (Figure 1). Subtype J increased from 3.5% in 1997 to 5.9% in 2015 [5, 6, 10]. The subtype K increased from 2.8% in 1997 and in 2002 to 9,8% in 2015 [5, 6, 8, 10]. The CRF02_AG, which was not presented the previous years in Kinshasa, is in the second position after subtype A [10]. This variant is becoming more and more important in Central Africa [17]. CRF02_AG is a recombined form of variants A and G [18]. These 2 subtypes were dominant in the past years in Kinshasa and even across the country [3]. Many wild-type strains are giving way to recombinant forms that escape more easily from ART [17]. These recombinations play a primordial role in the emergence of resistance to treatment [18]. The different strains which had a high prevalence in the past have decreased with time thus favoring the emergence of certain other subtypes such as subtype B, J, K, and CRF02_AG. These new variants are selected according to their adaptation to the cell environment, to the selection pressure exerted by the immune system and possibly to that exerted by the antiretroviral treatments [16].
CONCLUSION
The HIV epidemic in Kinshasa has been dominated by the Mgroup of HIV Type 1 since its 1983 declaration. The distribution of these circulating strains is constantly and dynamically evolving. Over the years, some subtypes have been confirmed while others have been erased due to pressure and different selections. The molecular HIV-1 epidemic in Kinshasa suggests persistence of subtype A and a significant increase in CRF02_ AG in the general population over time.
REFERENCES
- Ministry of Planning and Monitoring of the Implementation of the Revolution of Modernity, Ministry of Public Health and Democratic Republic of Congo (DRC). (2015). Demographic Health Survey (EDS-DRC).
- Robertson DL, Anderson JP, Bradac JA, Carr JK, et al. (2000). HIV Type 1 nomenclature proposal. Science. 288(5463): 55-56.
- Kamangu NE, Kabututu Z, Mvumbi LG, Kalala LR, et al. (2013). Genetic Diversity of Human Immunodeficiency Virus Type 1 in the Democratic Republic of Congo: a review of available data. International Journal of Collaborative Research on Internal Medicine and Public Health. 5(5): 295-309.
- Yang C, Dash B, Hanna SL, Frances HS, et al. (2004). The predominance of HIV Type 1 Subtype G among Commercial Sex Workers from Kinshasa, Democratic Republic of Congo. AIDS Research and Human Retroviruses. 17(4): 361-365.
- Mulanga-Kabeya C, Nzilambi N, Edidi B, Minlangu M, et al. (1998). Evidence of stable HIV seroprevalences in selected populations in the Democratic Republic of the Congo. AIDS. 12(8): 905-910.
- Vidal N, Peeters M, Mulanga-Kabeya C, Nzilambi N, et al. (2000). Unprecedented Degree of Human Immunodeficiency Virus Type 1 (HIV-1) Group M Genetic Diversity in the Democratic Republic of Congo Suggests that the HIV-1 Pandemic Originated in Central Africa. Journal of Virology. 74(22): 10498-10507.
- Yang C, Li M, Mokili LKJ, Winter J, et al. (2005). Genetic Diversification and Recombination of HIV Type 1 Group M in Kinshasa, Democratic Republic of Congo. AIDS Research and Human Retroviruses. 21(7): 661-666.
- Vidal N, Mulanga C, Delaporte E, Peeters M, et al. (2005). Distribution of HIV-1 Variants in the Democratic Republic of Congo Suggests Increase of Subtype C in Kinshasa Between 1997 and 2002. J Acquir Immune Defic Syndr. 40(4): 456-462.
- Djoko CF, Rimoin AW, Vidal N, Tamoufe U, et al. (2011). High HIV Type 1 Group M pol Diversity and Low Rate of Antiretroviral Resistance Mutations Among the Uniformed Services in Kinshasa, the Democratic Republic of the Congo. AIDS Research and Human Retroviruses. 27(3): 323-329.
- Kamangu NE, Chatté A, Susin F, Boreux R, et al. (2015). Genetic Diversity and Antiretroviral Drug Resistance among Drug-Naïve HIV Type 1 Infected Patients attending Clinics in Kinshasa, Democratic Republic of Congo. Journal of HIV and AIDS. 1(1)
- Mann M, Nzilambi N, Piot P, Bosenge N, et al. (1988). HIV Infection and Associated Risk Factors in Female Prostitutes in Kinshasa, Zaïre. AIDS. 2(4): 249-54
- Kamangu NE, Bongenia IB, Bulanda IB, Kalume AA, et al. Molecular and Virological Profile of Sex Workers and their partners at the beginning of ARV treatment at the IST Matonge Center in Kinshasa.
- Kamangu NE, Bulanda IB, Bongenia IB, Botomwito TH, et al. (2015). Virological Profile of Patients Infected with HIV Starting Antiretroviral Treatment in Kinshasa. Open Access Library Journal. 2: e1564.
- Kamangu NE, Kalala NH and Mesia G. (2012). Profile of Antiretroviral Treatment Centers in Kinshasa, Democratic Republic of Congo [Poster 388]. In Proceedings of the 1st International African Society of Laboratory Medicine (ASLM) Conference. 1-7.
- Buonaguro L, Tornesello ML, and Buonaguro FM. (2007). Human immunodeficiency virus type 1 subtype distribution in the worldwide epidemic: pathogenetic and therapeutic implications. J Virol. 81(19): 10209-10219.
- Hoetelmans RM. (1998). Sanctuary sites in HIV-1 infection. Antiviral therapy. 3(Suppl 4): 13-17.
- Peeters M, Toure-Kane C, and Nkengasong JN. (2003). Genetic Diversity of HIV in Africa: Impact on Diagnosis, Treatment, Vaccine Development, and Trials. AIDS. 17(18): 2547-2560.
- Moutouh L, Corbeil J and Richman DD. (1996). Recombination leads to the rapid emergence of HIV-1 dually resistant mutants under selective drug pressure. Proc Natl Acad Sci USA. 93(12): 6106-6111.