Previous Issues Volume 2, Issue 1 - 2018
Femoral Neck Stress Fracture in Elderly Population: A Case Report
Silvia Santiago Maniega, Hector J. Aguado, Blanca Ariño Palao, Ricardo León Fernández, Clarisa Simón Pérez, Gonzalo Martinez Municio, Miguel Angel Martín Ferrero
Hospital Clínico Universitario de Valladolid, Valladolid, Spain
Corresponding Author: Hector J. Aguado, Hospital Clínico Universitario de Valladolid, Valladolid, Spain, Tel: +34 696466002; Email: [email protected]
Received Date: 29 Jan 2018 Accepted Date: 04 Oct 2018 Published Date: 08 Oct 2018
Copyright © 2018 Aguado HJ
Citation: Aguado HJ, Maniega SS, Palao BA, Fernández RL, et al. (2018). Femoral Neck Stress Fracture in Elderly Population: A Case Report. M J Surg. 2(1): 011..
ABSTRACT
Femoral neck stress fracture (FNSF) is a rare cause of anterior hip pain and the diagnosis becomes difficult. The delay of diagnose can lead to complications such as displacement of the fracture or avascular necrosis of the femoral head. We report a case of an 83-year-old lady treated for lumbar and right inguinal pain. She did not report any traumatic event. Physical assessment was unspecific and hip and lumbar spine X-rays were normal so she was managed with pain killers. During the follow-up, seriated hip x-rays were normal. One year and a half after the pain started, the x-ray showed an incomplete FNSF, confirmed by MR.
The woman went under surgery for internal fixation of the fracture with a proximal femoral nail. She started weight-bearing immediately and inguinal pain disappeared. This case highlights the importance of clinical suspicion of this kind of fractures, especially when the x-ray is normal but the patient keeps complaining from inguinal pain.
KEYWORDS
Stress Fracture; Femoral Neck; Insufficiency Fracture; Fragility Fracture; Anterior Hip Pain.
ABBREVIATIONS
FNSF: Femoral Neck Stress Fracture. MR: Magnetic Resonance
INTRODUCTION
The repetitive and prolonged muscular activity on a bone that has not been adapted to this action, can produce a stress fracture. Etiologically, two types of stress fractures can be differentiated: fatigue fractures and insufficiency fractures. Fatigue fractures occur due to the application of abnormal muscular effort or torsion to a bone with normal characteristics. On the other hand, insufficiency fractures occur due to normal muscle activity applied on a bone with decreased mineral or elastic resistance [1].
Generally, there are 3 femoral locations susceptible to stress fractures: distal shaft, proximal shaft and femoral neck. The distal shaft (between the distal one-third and the femoral condyles) is a common site [2, 3]. There is also a relatively high incidence of proximal shaft fractures that occur primarily on the medial surface [3, 4]. The highest incidence rates of femoral stress fractures occur at the femoral neck [5-7] although other studies show comparable rates in femoral neck stress fractures (FNSF) and femoral shaft fractures (ranging from 1 to 7 percent of all stress fractures).
We present the case of an 83-year-old female treated of nonspecific lumbar and inguinal pain with a year follow-up and finally presenting with a FNSF. The FNSF was treated with a proximal femoral nail.
CASE REPORT
We present the case of an 83-year-old female with inguinal pain who had a past medical history of mild cognitive impairment, arterial hypertension, and hypercholesterolemia. She had had previous surgeries for diaphyseal radius fracture and total left knee arthroplasty due to femoral condyle necrosis.
The patient had been evaluated one year earlier for a right inguinal pain of mechanical characteristics. Physical assessment was unspecific: range of motion was complete and pain free with no shortening of the right lower limb. Inguinal palpation was painless. Pelvic radiographs showed a stage I-II right coxarthrosis ((Tönnis classification) [8,9]. The patient was managed with pain killers. The patient was referred again for consultation due to lumbar pain with irradiation to the right inguinal region. She referred an insidious mechanical lumbar and inguinal pain during the last months. She did not report any traumatic event nor a trigger factor for that pain. The physical assessment showed lumbar pain, and rotations of the hip were painless. The hip X-ray at that stage showed no signs of femoral neck fracture (Figure 1). The lumbar spine X-rays were also normal. She was prescribed treatment with nonsteroidal anti-inflammatory drugs and physiotherapy for the lumbar region.
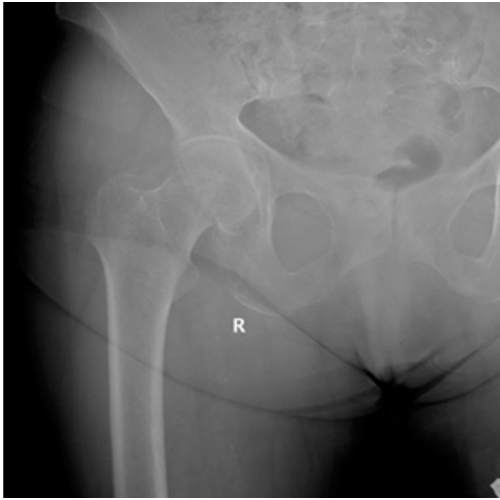
Figure 1: First visit right hip X- ray anteroposterior view. No signs of femoral neck fracture.
Four months later, the patient attended to the emergency room due to persistent inguinal pain. New hip X-rays were taken. Again, no sign of fracture was present. She was prescribed analgesic treatment and discharged home pending to be reevaluated at thespecialist’s office, leaving at his discretion the request for additional imaging tests (MR) not available at the emergency room.
One year and a half after the first visit in consultation, the pain was more intense and limited to the right inguinal region, despite the treatment. The patient showed mild physical impairment: she was using a cane for walking. The physical assessment showed hip stiffness: 90° of flexion, internal rotation of 5° and external rotation of 25°. The new hip X-ray showed an incomplete stress fracture in the middle of the superior aspect of the right femoral neck, located at the tension side (Figure 2). A hip MR confirmed the presence of an incomplete stress fracture of the right femoral neck. This fracture produced a decrease of the neck-shaft angle: (127o right side, 137o left side). There was also slight unexpected bone edema at the acetabulum roof level, probably caused by trabecular contusion (Figure 3).

Figure 2: Right hip X-ray: incomplete stress fracture in the middle of the superior aspect of the right femoral neck.
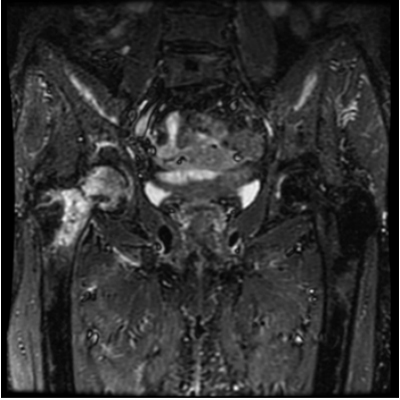
Figure 3: Coronal MR view confirms the presence of an incomplete stress fracture of the right femoral neck and bone edema at the acetabulum roof level.
The case was presented in clinical session deciding to fix the fracture with a proximal femoral nail. Surgical treatment was performed under spinal anesthesia on a traction table for surgeon comfort. No reduction was needed as the fracture was uncomplete. The fracture was fixed with a 10 mm proximal femoral nail (TFNA™, Depuy-Synthes, USA). Interfragmentary compression was done at the fracture site with the compression device of the nail system. Distal locking was applied. The operation lasted 30 minutes with no intraoperative incidents. Postop X-ray is shown in Figure 4. The day after the operation,the patient started walking with the help of a walker. She was discharged home without pain three days after the operation.
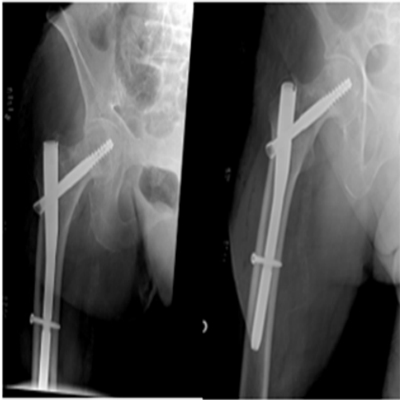
Figure 4: Post-op X-ray: intramedullary fixation with a proximal femoral nail.
DISCUSSION
Stress fractures may develop in up to 5% of runners and military trainers [10]. Of those patients who develop stress fractures, about 3-8% of the fractures are in the femoral neck [11]. In elderly patients, 16% of stress fractures occur in femoral neck [12]. Incidence of FNSF in elderly people is not well known, as most of FNSF reported in literature occur in young adults, especially military trainers and athletes [5, 10, 11, 13].
Intrinsic (non-modifiable) risk factors that contribute to stress fracture injuries include white race, female sex, amenorrhea, high bone turnover, low bone density, and inadequate muscle function [13]. Extrinsic (modifiable) risk factors that contribute to stress fracture injuries include overtraining, energetic nutrition deficit, vitamin D insufficiency, nicotine and alcohol abuse, steroid use, low adult weight, anorexia, or bisphosphonate therapy [14-16]. Many patients may present with a coexistence of different risk factors, which makes the isolation of etiologic variables difficult [17]. Inadequate diet and nutrition can also contribute towards the development of stress fractures. Smith et al. demonstrated an association between bone mineral density and veganism [18]. Vegans tend to have a lower intake of calcium and vitamin D, as well as a lower overall bone mineral density [18]. Our patient has some of the previously mentioned factors: she is an old frail lady with low bone density. She was also developing mild cognitive impairment, which can increase nutrition deficits, weight loss, and vitamin D insufficiency due to inadequate nutrition.
Fullerton and Snowdy [13] classified FNSF in three categories. The first category is defined as tension-side femoral neck fractures. In this category, the fracture line is placed in the superior part of the femoral neck. At the earliest stages, tensionside fractures have normal radiographs with positive bone scintigraphy on the tension side of the neck. The next stage exhibits either endosteal or periosteal callus on the tension side of the femoral neck or an overt tension-side fracture line without displacement. This stage is followed by widening of the tension-side fracture line. Finally, it appears that complete displacement of the femoral neck fracture is the end stage of the tension-side stress fracture [19]. The second category is defined as compression-side stress fracture, where the fracture line is seen in the inferior aspect of femoral neck. These fractures are more common than the previous category. Most commonly it exhibits sclerosis on the compression side of the femoral neck. The spectrum of radiographic changes starts with a negative radiograph with positive bone scintigraphy on the compression side of the femoral neck. The next, and most common stage is sclerosis without overt fracture [13]. It is followed by a compression-side cortical break, and then widening of the fracture line. The third category is when the fracture is already displaced in the initial X-ray and there is no evidence whether the fracture started originally in the tension side or in the compression side.
In our case, the patient presented tension-side stress fracture. We have almost followed the natural evolution of the fracture until reaching the diagnosis. In the first X-ray any sign of fracture was found, which can be the first stage of the fracture. The next X-ray showed cortical break on the tension side 10 months later. It is described that radiographic findings usually do not become apparent until 2 to 4 weeks after the onset of symptoms [20]. One of the peculiarities of this case is that radiographical signs of the FNSF started being visible months after the pain started. These findings allow us to ensure that at least during the first sixteen months in which the patient had pain, no sign of fracture was observed in the X-ray.
The earliest and most frequent symptom is anterior groin (inguinal) pain. On examination, pain at the extremes of hip range of motion is the most frequent and constant finding, followed by tenderness to palpation of the inguinal area overlying the hip joint [13]. In this case, the first symptom was lumbar and inguinal pain. As physical assessment was unusual and X-rays were unspecific, we could not find an etiologic cause for her pain. In the second visit, the patient only showed inguinal pain. We decided to take X-rays again because the physical assessment had changed, although it was still unspecific. The change in the physical assessment was correlated with a radiographic change.
The evolution of this case is longer than those presented in the literature [3, 21]. In spite of the long follow-up time, the fracture remained uncomplete. It did not evolve to a complete fracture nor a displaced fracture. For this reason, reduction of the fracture was not necessary during the surgery and the fracture could be fixed in situ.
FNSF are a rare cause of anterior femoral pain and the rule is a delay in the diagnosis. The average diagnostic delay is 14 weeks [22]. Patients are often being treated for muscle and tendon strains or early-onset coxarthrosis [23]. Hence high index of clinical suspicion must be maintained regarding all patients presenting with anterior hip pain without any significant trauma, especially when presenting symptoms are out of proportion to the radiological picture of degenerative changes. As the treatment aims mainly to reduce the pain and sustain patients’ activity level, this may lead to fracture displacement and following complications.
The blood supply to the femoral head runs through the femoral neck; thus, an FNSF may disrupt the blood supply to the femoral head and cause avascular necrosis of the femoral head [24].
The definitive treatment of the stress fracture can be conditioned by the presence of displacement of the fracture or avascular necrosis. In these cases, treatment with hip arthroplasty can be indicated. When an early diagnosis is made, and the fracture is not displaced, fracture fixation may be considered either with cannulated screws or intramedullary femoral nailing. In this case nor fracture displacement neither signs of avascular necrosis were present, thus fixation was the indicated treatment.
The learning point of our case report is that all cases of anterior hip pain are not due to early onset osteoarthritis. Other differential diagnosis, including stress fracture and avascular necrosis, should be considered in patients with minimal radiological evidence of osteoarthritis. Our patient had severe hip pain out of proportion to the clinical and radiological findings. Over one year, the patient was diagnosed of coxarthrosis and lumbar pain due to the absence of clear radiographic signs of fracture. It is important to keep in mind SFNF as differential diagnosis of anterior hip pain, especially when the patient has risk factors that contribute to this kind of fractures such as the case we present.
However, the most important factors for a correct diagnosis are: regular follow up with regular radiographic review [25,26] and awareness of this rare cause of anterior hip pain.
Thanks to close follow-up through radiographs, an early treatment of the fracture could be considered in our case. The patient underwent intramedullary nailing, a non-aggressive surgery, with short hospitalization time, that allowed immediate weight bear, all suitable for this frail patient.
REFERENCES
- Egol KA, Koval KJ, Kummer F and Frankel VH. (1998). Stress fractures of the femoral neck. Clin Orthop Relat Res. 348: 72-78.
- Niva MH, Kiuru MJ, Haataja R and Pihlajamaki HK. (2005). Fatigue injuries of the femur. J Bone Joint Surg Br. 87(10): 1385-1390.
- Korpelainen R, Orava S, Karpakka J, Siira P, et al. (2001). Risk factors for recurrent stress fractures in athletes. Am J Sports Med. 29(3): 304-310.
- Fredericson M, Jennings F, Beaulieu C and Matheson GO. (2006). Stress fractures in athletes. Top Magn Reson Imaging. 17(5): 309-325.
- Pentecost RL, Murray RA and Brindley HH. (1964). Fatigue, Insufficiency, and Pathologic Fractures. JAMA. 187: 1001-1004.
- Markey KL. (1987). Stress fractures. Clin Sports Med. 6: 405-425.
- Tonnis D. (1987). Congenital dysplasia and dislocation of the hip in children and adults. Berlin: Springer.
- Clohisy JC, Carlisle JC, Sierra RJ, Beaule PE. et al. (2008). A Systematic Approach to the Plain Radiographic Evaluation of the Young Adult Hip. The Journal of Bone and Joint Surgery American. 90(4): 47-66.
- Amstrong DW 3rd, Rue JP, Wilckens JH and Frsassica FJ. (2004). Stress fracture injury in young military men and women. Bone. 35(3): 803-816.
- Pihlajamaki HK, Ruohola JP, Weckstrom M and Kiuru MJ. (2006). Long-term outcome of undisplaced fatigue fractures of the femoral neck in young male adults. J Bone Joint Surg Br. 88(12): 1574-1579.
- Carpintero P, Berral FJ, Baena P, Garcia-Frasquet A, et al. (1997). Delayed diagnosis of fatigue fractures in the elderly. Am J Sports Med 25(5): 659-662.
- Fullerton LR Jr and Snowdy HA. (1988). Femoral neck stressfractures. Am J Sports Med. 16(14): 365-377.
- Breer S, Krause M, Marshall RP, Barvencik F, et al. (2012). Stress fractures in elderly patients. Int. Orthop. 36(12): 2581-2587.
- Koh JS, Goh SK, Png MA, Kwek EB, et al. (2010). Femoral cortical stress lesions in long-term bisphosphonate therapy: a herald of impending fracture? J Orthop Trauma. 24(2): 75-81.
- Isaacs JD, Shidiak L, Harris IA and Szomor ZL. (2010). Femoral insufficiency fractures associated with prolonged bisphosphonate therapy. Clin Orthop Relat Res. 468(12): 3384-3392.
- Ben Chihaoui M, Elleuch M, Sahli H and Cheour I, et al. (2008). Stress facture: epidemiology, physiopathology and risk factors. Tunis Med. 86(12): 1031-1035.
- Smith AM. (2006). Veganism and osteoporosis: a review of the current literature. Int J Nurs Pract. 12(5): 302-306.
- Devas MB. (1965). Stress fractures of the femoral neck. J Bone Joint Surg. 47B: 728-738.
- Boden BP and Speer KP. (1997). Femoral stress fractures. Clin Sports Med 16(12): 307- 317.
- Onibere OA and Sugathan HK. (2015). A case report of missed femoral neck stress fracture. SICOT J. 1: 2.
- Avrahami D and Pajaczkowski JA. (2012). Femoral neck stress fracture in a female athlete: a case report. Journal of Chiropractic Medicine. 11(4):273-279.
- Johansson C, Ekenman I, Tornkvist H, and Eriksson E. (1990). Stress fractures of the femoral neck in athletes. The consequences of a delay in diagnosis. Am J Sports Med. 18(5): 524-528.
- O'Kane JW. (1999). Anterior hip pain. Am Fam Physician 60(6): 1687-1696.
- Lee C, Husng GS, Chao KH, Jean JL, et al. (2003). Surgical treatment of displaced stress fractures of the femoral neck in military recruits: a report of 42 cases. Arch Orthop Trauma Surg. 123(10): 527-533.
- Clough TM. (2002). Femoral neck stress fracture: the importance of clinical suspicion and early review. Br J Sports Med 36(4): 308-309.
- Fullerton LR Jr. (1990). Femoral neck stress fractures. Sports Med 9(3): 192-197.