Previous Issues Volume 1, Issue 2 - 2017
A Rare Presentation of Acute Abdomen due to Intersigmoid Hernia Successfully Treated by Laparoscopic Surgery
Yoshimasa Kishi1 , Tetsuya Yumoto1 , Kohei Tsukahara1 , Atsuyoshi Iida1 , Satoru Kikuchi2 , Shinji Kuroda2 , Hiromichi Naito1 , Yasuaki Yamakawa1 , Toshiyoshi Fujiwara2 , Atsunori Nakao1*
1Department of Emergency and Critical Care Medicine, Okayama University Graduate School of Medicine Dentistry and Pharmaceutical Sciences.
2 Department of Gastrointestinal Surgery, Okayama University Graduate School of Medicine Dentistry and Pharmaceutical Sciences
Corresponding Author: Atsunori Nakao, Department of Emergency and Critical Care Medicine, Okayama University Graduate School of Medicine Dentistry and Pharmaceutical Sciences, 2-5-1 Shikata-cho, Kita-ku, Okayama-shi, Okayama, 700-8558, Japan.
Tel: +81-78-241-3131; Email: [email protected]
Received Date: 07 Feb 2017 Accepted Date: 21 Feb 2017 Published Date: 27 Feb 2017
Copyright © 2017 Nakao A
Citation: Kishi Y, Yumoto T, Tsukahara K, Nakao A, et al. (2017). A Rare Presentation of Acute Abdomen due to Intersigmoid Hernia Successfully Treated by Laparoscopic Surgery. Mathews J Surgery 1(2): 005.
ABSTRACT
A 56-year-old man with no previous medical history was transferred by ambulance to local hospital with acutely onset abdominal pain. Computed tomography demonstrated ileum loop in the left iliac fossa, suggesting intersigmoid herniation of ileum with intestinal strangulation. Emergency laparoscopic surgery was performed and incarcerated ileum was reduced from the hernia orifice. Since the strangulated intestibe was viable, no intestine was resected. His postoperative course was uneventful. Diagnosis of acute abdomen caused by intersigmoid hernia remains difficult preoperatively. The emergency physician should keep in mind the possibility of intersigmoid hernia in a patient with acute-onset abdominal pain even with no vomiting or bowel obstruction. Laparoscopic exploration may offer decisive information and thereby prevent delays in providing definitive treatment.
INTRODUCTION
Laparoscopic surgery for acute abdomen has become widely accepted in the emergency medicine, and already proved its safety and feasibility in the selected cases [1, 2]. Compared to open surgery, the greatest advantages of laparoscopy include faster recovery times, shorter hospital stays and decreased postoperative pain, as well as cosmetic benefits. Herein, we report a case of intersigmoid hernia of ileum loops presenting acute abdomen, successfully treated by laparoscopic surgery. The pathogenesis of intersigmoid hernia involves herniation of a small bowel through the intersigmoid fossa, a recess located at the level of the iliac crest where the descending colon becomes the sigmoid colon and acquires a mesentery. Although the overall incidence of intersigmoid hernia is low, they account for significant mortality from intestinal strangulation. Our report showing typical radiological images may help the emergency physician to make an accurate diagnosis and make the most appropriate strategy for treatment of the patient.
CASE REPORT
A 56-year-old man was admitted to our hospital with 5 hours history of intermittent and cramping pain in the left lower abdomen. He had no history of any abdominal surgery. On arrival, his vital signs include body temperature of 36.7°C, blood pressure of 143/96 mmHg, heart rate of 109/min and respiratory rate 22/min. No vomiting or diarrhea was present. The abdomen was slightly distended with rebound tenderness and rigidity over left lower quadrant. There was no evidence of organomegaly or superficial lymphnode swelling. His external hernia orifices were normal. Laboratory examinations showed leukocytosis (17500/mm3 ) and elevated C-reactive protein (0.17 mg/dL) without abnormal value of liver function or renal function.
Contrast-enhanced computed tomography (CT) of the abdomen and pelvis disclosed was thickening of the edematous, fluid-filled ileum loop with poorly contrast-enhanced in the left iliac fossa. We had a diagnosis as internal hernia or fibrous bands and planned the laparoscopic exploration. Under gen-eral anesthesia, the laparoscope was inserted via infraumbilical 12mm trocar, and two of 12mm ports were placed. The intraoperative diagnosis was an intersigmoid hernia. Approximately 50 cm of loop of ileum incarcerated in the sigmoid fossa and strangulated. Small intestine demonstrated features of slight ischemia but viability and therefore was not resected. His postoperative course was uneventful. The patient was discharged on postoperative day 3.
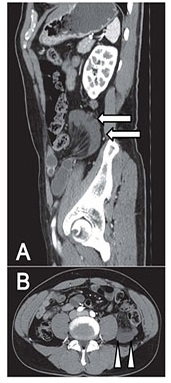
Figure 1: Computed tomography A. Computed tomography showed wall thickening of the edematous, fluid-filled ileum in the left iliac fossa and pelvic cavity (arrow). B. An incarcerated jejunal loops (arrowhead) is located anterior to the left psoas muscle.
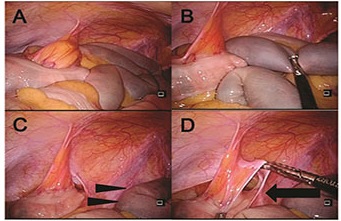
Figure 2: Intraoperative findings. A. Approximately 50 cm of loop of ileum incarcerated in the sigmoid fossa and strangulated. B. Loop of the ileum is taken out from the hernia orifice. C. Incarcerated small intestine demonstrated features of slight ischemia but viability(arrowhead). D. Hernia orifice is indicated by black arrow.
DISCUSSION
Internal hernias is protrusion of viscous or part of a viscous through anatomical or pathological opening within the limits of peritoneak cavity, including paraduodenal, perocecal, through foramen of Winslow, mesocolon and retroanastomotic hernias. Sigmoid mesocolon hernias are classified into three types, intersigmoid hernia, transmesosigmoid hernia and intermesosigmoid hernia, and together they represent around 6% of all internal hernias [3]. Intersigmoid hernia, the most common type, is herniation into a congenital fossa, the intersigmoid fossa, situated in the attachment of the lateral aspect of the sigmoid mesocolon.
The clinical signs and symptoms of intersigmoid hernia are non-specific including abdominal pain, nausea, vomiting and distension. The most common clinical presentation is bowel ischemia with some degree of bowel obstruction. However, if hernias are easily reducible, the clinical presentation may be intermittent or transient [4]. An urgent abdominal CT scan is useful for the diagnosis of intersigmoid hernia and can help to minimize strangulation, conserve bowel and reduce patient morbidity and mortality. Understanding the anatomy of the peritoneal cavity and the characteristic anatomic location of each internal hernia, as well as recognition of the characteristic CT findings, may assist in consideration or identification of internal hernias in most cases of acute abdomen [5].
The therapeutic strategy for intersigmoid hernia is either a reduction or resection of the herniated intestine, as well as closure of the defect by surgery. Prompt surgical intervention is generally warranted in patients with suspected internal hernias. As with our patient, laparoscopy is an excellent option in diagnosing and treating the internal hernia patients. Using advanced laparoscopic skills, the cause can be confirmed, and frequently unexpected pathology can be addressed. Laparoscopy must be reserved for hemodynamically-stable patients in selected cases.
CONCLUSION
Emergency physicians should suspect an internal hernia in patients presenting acute obstruction, no past surgical history and no external hermia, even in the absence of characteristic radiological findings. The laparoscopic approach is ideal in hemodynamically stable patients with intersigmoid hernia who do not have extensive prior abdominal surgeries.
ACKNOWLEDGEMENT
The authors would like to acknowledge Ms Christine Heiner who reviewed and edited the manuscript.
REFERENCES
- Mandrioli M, Inaba K, Piccinini A, Biscardi A, et al. (2016). Advances in laparoscopy for acute care surgery and trauma. World J Gastroenterol. 22(2): 668-680.
- Agresta F, Campanile FC, Podda M, Cillara N, et al. (2016). Current status of laparoscopy for acute abdomen in italy: A critical appraisal of 2012 clinical guidelines from two consecutive nationwide surveys with analysis of 271,323 cases over 5 years. Surg Endosc.
- Benson JR and Killen DA. (1964). Internal hernias involving the sigmoid mesocolon. Ann Surg. 159(3): 382-384.
- Nihon-Yanagi Y, Ooshiro M, Osamura A, Takagi R, et al. (2010). Intersigmoid hernia: Report of a case. Surg Today. 40(2): 171-175.
- Takeyama N, Gokan T, Ohgiya Y, Satoh S, et al. (2005). Ct of internal hernias. Radiographics. 25(4): 997-1