Previous Issues Volume 1, Issue 1 - 2016
Medical Trainee Designation: Staff Confusion and Potential Impact on Patients & Training
Farshad Shaddel1, Marjan Ghazirad2, Denis O'Leary3
1Consultant Psychiatrist, Berkshire Health NHS Foundation Trust, UK.
2Psychiatry Specialist Registrar, Oxford Deanery, UK.
3Honorary Clinical Tutor, Medical Sciences Division, University of Oxford, UK.
Corresponding Author: Farshad Shaddel, MRCPsych, SFHEA, Consultant Psychiatrist in Learning Disability, Oxford University Medical Education Fellow, Senior Fellow of the Higher Education Academy, UK. Tel: 0113 2955432; E-Mail: f_shaddel@yahoo.
Received Date: 6 Jun 2016 Accepted Date: 15 Jun 2016 Published Date: 20 Jun 2016
Copyright © 2016 Shaddel F
Citation: Shaddel F, Ghazirad M and O'Leary D. (2016). Medical Trainee Designation: Staff Confusion and Potential Impact on Patients & Training. Mathews J Psychiatry Ment Health. 1(1): 004.
ABSTRACT
Introduction: The complexity of new terms for UK trainee doctors has raised concerns for patient safety and teamworking. Older terms (junior or resident) may compound these effects. This study explores other team-members': (i) understanding of the new terminology; (ii) accuracy of matching clinical tasks to the core training grade; and (iii) attitudes to the term "junior".
Methods: Fifty staff from two psychiatric healthcare providers were surveyed. Respondents selected the doctor grade they would ask to complete 8 clinical tasks, chosen from competencies expected of the core training grade. Experience based models of training provided the conceptual framework.
Results: Only 14% self-rated as having a partial or complete understanding of the new terms. Signposting of clinical tasks was mismatched to the core trainee grade. Up to 10% signposted more complex tasks to training grades above their competency expectations. The term "junior" was negatively perceived and linked to requests for more senior input.
Discussion: The results support findings that only 22% of surgical nurses fully understood the new terminology; they extend them by demonstration of risks to patient care and reduced training opportunities. National training bodies and employers considering changes to terminology should ensure steps to address these risks.
KEYWORDS
Trainee Terminology; Training Opportunities; Patient Safety.
INTRODUCTION
BACKGROUND
Since 2007 in the UK an increased number of terms have been used by General Medical Council (GMC) in the UK to classify grades of doctors in psychiatry training to reflect the international shift toward competency based medical education. Terms such as Specialist Registrar/Higher Trainee (ST4-6), Specialty Registrar/Core Trainee (CT1-3), Foundation Doctor (FY1-2) have replaced the older and well established terms such as Registrar (SpR), General Practice Vocational Training Scheme (GPVTS), Senior House Officer (SHO) and House Officer (HO). Faced with such complexity the default term "junior doctor" has been used widely instead [1]. However a default term (e.g. "Resident") may cause confusion too as US studies report [2]. As far as we are aware the situation has not changed as yet. Educationally and independent of any impact on the trainee's self-efficacy, a default (generic) term is likely to limit training opportunities and patient care - through mismatching of clinical tasks and trainee competency levels. The aims of this study, undertaken within a single specialty (psychiatry), were to explore other healthcare professionals': (i) understanding of the different terms by which doctors in training are designated; (ii) how well they could match clinical tasks to a specific (i.e. core training) grade; and (iii) their attitude to the term "junior".
METHODS
The survey was conducted by interviews of staff (non-medical) from two health providers providing psychiatry training posts in Oxford. The design included a simple stratified sample of staff working with trainees at randomly selected wards or community teams. The interview tool consisted of closed and open questions (appendix1). Staff were asked to select from seven medical categories (lowest training grade to consultant) and one "Other Professional" category, the person they would ask to undertake specified clinical tasks. These tasks were expected learning outcomes from the core training programme curriculum chosen as its competency requirements are intermediate between Foundation, General Practice, and Higher Training grades [3]. The tasks included the overall performance expected of a trainee at the end of the programme and seven items related to less complex curricular outcomes. To minimise bias interviewees were not informed about the links to the core curriculum. Two additional items explored interviewees responses to the term "junior" using a vignette-based approach and finally their agreement along a Likert scale with the statement: "I am clear about the role and competency of different doctors" [4]. They were asked for any linked recommendations arising from this item. The interviews were conducted between February - July 2013 by FS and MG following a small pilot study to match their interview style. The survey was registered with the relevant audit office and approval obtained from the medical education leads at hospital and training authority level. Formal ethics committee approval was not required as per National Research and Ethics Service guidelines and no patients were interviewed [5]. Consent to the face-to-face interview was obtained from each staff member prior to any rating of the survey items. There was no time limit for respondents' replies which were recorded on an anonymised basis.
RESULTS
All intended sites (10 inpatient wards and 7 community teams) agreed to participate; 50 staff were approached for interview; none declined and all completed the survey. Thirty two (64%) were nurses and 31 (62%) were community based.
Responses to Clinical Task signposting
Staff were asked to identify the category of doctors they considered "Safe to make decisions in all but the most complex clinical situations; competent"- the core training programme end outcome. The results are presented in Table 1 (with some categories collapsed into a "ther Doctors" category due to small numbers). This group contains doctors who are in training grades below that of Core trainees and non-training grades below or equivalent in competency with Core trainees). Only 20% chose the Core trainee grade; the majority (68%) chose more senior grades while 10% chose the category for whom the task is outside their curricular requirements or clinical experience.
Table 1:Signposting to medical categories by respondents (n=50) to different doctors.
| Task to be signposted | Level of Grade Seniority | Other Professionals | |||
|---|---|---|---|---|---|
| Other Doctors* | Core Trainee | Higher Trainee | Consultant | ||
| Safe/competent in all but most complex situations | 5 (10%) | 10 (20%) | 21 (42%) | 13 (26%) | I (2%) |
| Psychiatric history taking and MSE | 30 (60%) | 6 (12%) | 10 (20%) | 3 (6%) | 1(2%) |
| Recommend the management plan | 17 (34%) | 2 (4%) | 13 (26%) | 17 (34%) | 1 (2%) |
| Assessment of risk to self/ others | 25 (51%) | 4 (8%) | 13 (27%) | 2 (4%) | 5 (10%) |
| Psychological treatments | 10 (20%) | 8 (16%) | 12 (25%) | 3 (6%) | 16 (33%) |
| Record keeping | 37 (74%) | 3 (6%) | 2 (4%) | 1 (2%) | 7 (14%) |
| Assessment & management of chronic and enduring mental illnesses | 10 (20%) | 4 (8%) | 11 (22%) | 24 (48%) | 1 (2%) |
| Communicating with patient/relatives | 36 (72%) | 1 (2%) | 3 (6%) | 3 (6%) | 7 (14%) |
*Foundation trainees (FT); GPVTS; Trust Doctors (TD); Junior Doctors (JD).
Regarding the more specific core training curricular competencies, the percentage of respondents who identified these as Core trainee' tasks ranged from 2 to 16%. In contrast the percentage range for the Other Doctors category was higher (20-74%) with the actual percentage being so across each task. The differences being particularly noticeable for taking a history/MSE, enduring mental illness and record keeping. The percentage of respondents opting for other professionals over Core trainees was highest across psychological treatments.
Vignette Responses
In response to the vignette-based item "Your car will be tested and repaired by our "Junior technician" only 30% chose the "I do not mind" option; the remainder chose either to seek clarification about the competency of the junior technician or a more qualified technician /second opinion (Figure 1). When asked to expand on their response they referred to the term "junior"as indicating: "Incompetency", "Lack of experience" and "Inadequacy". One staff member interpreted it as a "Baby professional" who "should be looked after".
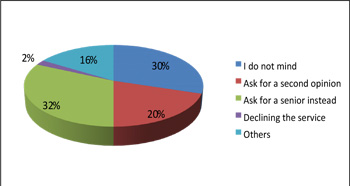
Figure 1:Respondents' responses to "Junior technician".
Understanding of Training Grade Terminology When asked to rate their understanding of current training terminology 14% indicated a fully or partially clear understanding (Figure 2).
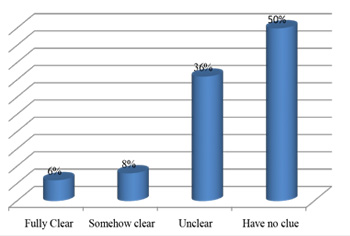
Figure 2: Staff Clarity on Doctor in Training terminology.
Respondents' suggestions for improved understanding included:
- Providing documentation on the competency levels of different doctors (poster, email or other) - 44%
- Better and more meaningful terminology to describe doctors' competency levels and avoidance of repeated changes to the terminology (27%)
- Better individual introduction of the doctor on joining the team that clarifies their experience and expected competence level (20%) 4. Training sessions (9%).
DISCUSSION
Within health teams, reciprocal understanding of the roles of all health professionals enhances team working and patient care [6]. Training opportunities within teams motivate trainees' learning through promotion of clinical expertise and professional identity; facilitation of any healthcare professional's training therefore requires knowledge of their competency levels by other team members [7, 8]. In practice such knowledge is usually understood in terms of training grade terminology. Our findings show that 14% of respondents self-rated as having a partial or full understanding of medical training grade terminology, supporting a similar finding (22% of 55 nurses) in a surgical setting. Together the reports tend towards a generalisation of findings across specialties and show that lack of clarity may persist for several years (six in the current report). Findings from the US show that poor clarity extends to patients even without any changes in complexity to the medical grade designations [2]. An original feature of this study is the confirmation of the earlier report's implication of how poor understanding of medical grade terminology could cause harm to patients [1]. In up to 10% of instances the more complex tasks were signposted to training grades where such complexity was above their expected curricular requirements. Such mismatching if repeated in the workplace may be a contributing factor to actual errors by doctors transitioning across training grades [9]. In addition to the patient safety aspects, the findings show how poor understanding of training grade terminology could result in reduced opportunities for training - either through referral to more senior grades (as in the more complex tasks) or to Other Doctors or Professionals for less complex tasks. The former, in addition to reducing training opportunities, is likely to compound the workload of more senior doctors already working to new legal working directives and increased service demand [10]. Additionally It is possible that signposting of curricular inappropriate tasks to higher grades may lie in respondents' beliefs in the term "junior" - which the findings show, even in a non-medical context, was linked by respondents to a perceived lack of competence. The situation is compounded if more curricular appropriate tasks are directed away from the specific training grade in addition. The limitations of the study include the choice of a single specialty and only two healthcare providers, thus limiting generalisation; and the relative delay in reporting these results. However the changes in training grade terminology in the UK are not confined to psychiatry, and there is similarity of results with a very disparate specialty (surgery) as noted above. Furthermore the issues arising from changes to trainee terminology remain current given the shift internationally towards competency based medical education and linked trainee designation. To address these issues (risks to patient care, reduced training opportunities, increased senior doctor workload) we support patient (and in this study staff) requests for more information on training grade terminology in the workplace. In addition we recommend that national bodies considering changes to how doctors in training are titled consider the impact on other team members' practical understanding of the new terms and the impact on patient care, given the length of time that may otherwise be required to embed these changes.
REFERENCES
- Islam S, Deekes A, Lee A, Isgar B, et al. (2011). Junior doctor titles following implementation of Modernising Medical Careers in the UK, JRSM Short Rep. 2(3), 22.
- American Medical Association, Survey Results. 2008 and 2010.
- A Competency Based Curriculum for Specialist Core Training in Psychiatry, Royal College of Psychiatrists. 2010.
- Wuensch K. (2015). What is a Likert Scale? and How Do You Pronounce 'Likert? East Carolina University. Retrieved.
- National Research Ethics Services (http://www.nres.nhs. uk/)
- Dornan T, Boshuizen H, King N, Scherpier A, et al. (2007). Experience-based learning: a model linking the processes and outcomes of medical students' workplace learning. Med Educ. 41(1), 84-91.
- Doyle J. (2008). Barriers and facilitators of multidisciplinary team working: a review. paediatric nursing. 20(2), 26-29.
- Ericson KA. (2004). Deliberate practice and acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 79 (10 suppl), 70-81.
- McLay J and Ross S. (2008). Medication errors caused by junior doctors. BMJ. 336(7642), 456.
- Shaddel F and Banerjee S. (2013). Impact of the European Working Time Directive on trainees and trainers 3 years postimplementation. Psychiatric Bulletin. 37(9), 286-289.