Previous Issues Volume 1, Issue 1 - 2018
A Simple Voice Training Method by Emphasizing Abdominal Respiration and Refractory Laryngeal Granulomas
Takeshi Kusunoki1*, Katsuhisa Ikeda
1Department of Otorhinolaryngology,Juntendo University of Medicine, Shizuoka Hospital.
2Department of Otorhinolaryngology, Juntendo University Faculty of Medicine.
Corresponding Author: Takeshi Kusunoki, Department of Otorhinolaryngology, Juntendo University of Medicine, Shizuoka Hospital, 1129 Nagaoka Izunokuni-shi, Shizuoka 410-2295, Japan, Tel: +81-55-948-5088; E-Mail: [email protected]
Received Date: 03 Sep 2017 Accepted Date: 07 Oct 2017 Published Date: 10 Oct 2017
Copyright ©2017 Kusunoki T
Citation: Kusunoki T and Ikeda K. (2017). A Simple Voice Training Method by Emphasizing Abdominal Respiration and Refractory Laryngeal Granulomas. M J Otol. 1(1): 002.
ABSTRACT
Background: Previously, we designed a simple method of voice training by emphasizing abdominal respiration and our voice therapy was reported to improve most cases with vocal fold nodules or polyps. Some hospitals reported that operation and proton pump inhibitors (PPI ) were not very effective for laryngeal granulomas. In this study, our voice training method was employed for refractory laryngeal granuloma cases with resistance to PPI(including some operative recurrent cases before or after PPI treatment).A male child 6 year old presenting acutely, following trauma, with the clinical appearance of a right nasal mass appearance like 'blueberry' within the right nasal vestibule since 7 days. We recommend early surgical drainage and excision of this lesion, as delay in definitive treatment may give rise to a cosmetic deformity.
Subjects and Methods: All 29 cases of laryngeal granuloma had not improved with PPI treatment for 8 weeks. Some cases underwent laryngomicrosugery before or after PPI treatment and showed postoperative recurrence. All cases were treated by our method of voice training alone, using no other therapy (e.g., silence therapy, medicine, operation) during the voice training period.
At our hospital otorhinolaryngology out-patient clinic, voice therapy was performed using a simple method of voice training by emphasizing abdominal respiration. In additional to the home exercise program, all patients received a detailed explanation of our voice training method, and exercised twice or three times-daily for 10 minutes. Moreover, we instructed them as follows. If patients sense that phonation during daily conversation excessively stresses the vocal fold, they should correct to naturally relaxed phonation by exhaling with abdominal respiration. Follow up evaluations were scheduled for every month after their initial visit.
Results: In 26 of 29 cases with laryngeal granulomas, the lesions disappeared or reduced.
Conclusions: These results suggest that our method of voice training could improve many cases with refractory laryngeal granuloma.
KEYWORDS Abdominal Type of Respiration; Voice Training; laryngeal Granuloma; Proton Pump Inhibitor (PPI).
INTRODUCTION
It has been suggested that doctors should perform voice therapy in cooperation with speech therapists [1]. However, speech therapists have not fully spread in Japan. Therefore, we designed “a simple method of voice training by emphasizing the importance of abdominal respiration” and relying on only a single doctor to administer this voice training. Voice therapy is the first choice for vocal fold nodules in Japan [2]. Previously, we reported the improvement of 9 cases with vocal fold nodules using this method [3].
Some hospitals reported high rates of postoperative recurrence, therefore, proton pump inhibitor (PPI ) treatment have been the first choice for laryngeal granulomas. However, some cases do not improve by PPI alone [4]. In this study, our voice training was employed for refractory laryngeal granuloma cases that were resistant to PPI (including postoperative recurrent cases ).
In Japan, evaluation of the effectiveness of voice therapy is widely done using the grade rough breathy asthenic strained scale (GRBAS scale) [4]. The GRBAS scale is considered the gold standard for psychoacoustic voice evaluation in Japan, and is a subjective rather than objective evaluation. Therefore, we tried to make our evaluation as objective and clear as possible. The grade of the effectiveness of our training was evaluated by changing the laryngeal diseases.
METHODS
At our hospital otorhinolaryngology out-patient clinic, voice therapy was performed from April 2011 to June 2017 using the simple method of voice training by stressing the importance of using abdominal respiration. All patients (29) received an explanation about surgical and pharmacological treatments, as well as our voice training method, and chose our method of voice training. Finally, All 29 cases with laryngeal granulomas had not improved by PPI treatment for 8 weeks. Four cases with postoperative recurrence did not improve by PPI treatment. All cases were treated by our method of voice training alone, using no other therapy (e.g., silent therapy, medicine, operation) during the voice training period.
In our method of voice therapy, new patients were instructed to master the abdominal type of respiration at the first medical examination as follows [2]. Patients practiced exhaling from the mouth with inward abdominal movement and inhale nasally with outward abdominal movement while relaxing the upper half of the body. Next, patients practice voice training with naturally relaxed phonation using first “f” and gradually changing from “f” to“v”, while exhaling with abdominal respiration. Our voice training is intended to avoid excessive stress of the vocal fold due to inadvertently strong laryngeal phonation. In additional to the home exercise program, all patients received a detailed explanation of our voice training method, and exercised twice or three times-daily for 10 minutes. Moreover, we instructed them as follows. If patients sense that phonation during daily conversation excessively stresses the vocal fold, they should correct to naturally relaxed phonation by exhaling with the abdominal type of respiration. Follow up evaluations were scheduled for every month after their initial visit.
The evaluation grade of the therapy effectiveness for laryngeal disease itself was classified into three types as follows “disappearance”, “reduction”, “no change”. Concerning the criterion for “reduction”, the diseased volume is less than one-half of that before voice therapy.
RESULTS
On laryngeal granulomas, the chief complaint in 9 of 29 cases was hoarseness. 8 of 29 cases had no pharyngo-laryngeal symptoms, although they had occasionally shown laryngeal granulomas by upper gastrointestinal endoscope or laryngoscope. In twenty-six of 29 cases with laryngeal granulomas, the lesions disappeared (18) or reduced (8) by our method of voice training (Table 1).
Table 1: Averages of the characteristics of the group and relationship with physical activity for each genus and the total sample.
| Case | Motivation for consultation | Operation | Period of voice training | Effectiveness |
| 60 years M | hoarseness | 9 months | reduction | |
| 70 years M | point out by GIF | 7 months | reduction | |
| 45 years M | point out by GIF | 16 weeks | reduction | |
| 50years M | throat discomfort | 7 weeks | disappearance | |
| 70 years M | point out by GIF | 3 weeks | disappearance | |
| 62 years M | point out by GIF | 7 months | reduction | |
| 62 years M | hoarseness | 8 weeks | reduction | |
| 64 years M | throat discomfort | 16 weeks | disappearance | |
| 42 years M | throat discomfort | 9 months | no change | |
| 70 years F | hoarseness | 5 weeks | disappearance | |
| 68years M | point out by GIF | 3 months | disappearance | |
| 56 years M | throat discomfort | 2 months | no change | |
| 60 years M | point out by GIF | 4 months | reduction | |
| 67 years F | hoarseness | 3 months | no change | |
| 56 years M | throat discomfort | 6 months | no change | |
| 63 years M | hoarseness | 3 months | disappearance | |
| 58 years M | throat discomfort | 2 months | disappearance | |
| 76 years M | throat discomfort | + | 2 months | disappearance |
| 73 years M | hoarseness | + | 1 months | disappearance |
| 75 years M | hoarseness | 2 months | disappearance | |
| 45 years F | hoarseness | 4 months | disappearance | |
| 66 years M | throat discomfort | 4 months | disappearance | |
| 53 years M | throat discomfort | + | 3 months | disappearance |
| 41 years M | throat discomfort | 3 months | disappearance | |
| 59 years M | throat discomfort | + | 4 months | reduction |
| 38 years M | point out by laryngoscope | 3 months | no change | |
| 56 years M | point out by GIF | 10 months | disappearance | |
| 48 years M | 2 months | reduction | ||
| 62 years M | throat discomfort | + | 3 months | disappearance |
M: Male F: Female GIF: gastrointestinal endoscope
Some cases with hyperfunctional dysphonia at the first medical examination showed improvement by our method of voice training together with reduced anterior-posterior contraction of the larynx (Figure 1).
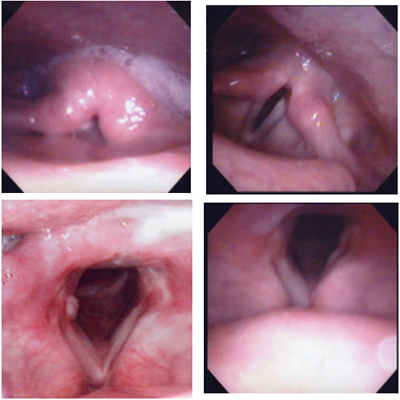
Figure 1: Endoscopic finding of laryngeal granulomas (Case No 16 in table 1).

Figure 2:CT image of nasal swelling.
Left: Laryngeal granuloma case with hyperfunctional dysphonia at the first medical examination showed severe anterior-posterior contraction resulting in contact between the aryteoid and laryngeal side of the epiglottis.
Right: Our method of voice training for 3 months caused the laryngeal garnuloma to disappear and improved the hyper-functional dysphonia, while reducing the anterior-posterior contraction of the larynx.
Four cases with postoperative recurrence could not be improved by PPI treatment, but the lesions disappeared after using our voice training method (Figure 2).
Lower left: A laryngeal granuloma at first examination Lower left: This laryngeal granuloma was removed by laryngomicrosurgery Right upper: A recurrent laryngeal granuloma appeared at one and a half years after the operation. Lower right: This postoperative recurrent laryngeal granuloma disappeared after using our voice training method for two months.
Most patients that could master the abdominal respiration in the laryngeal granuloma showed improvements and were able to speak comfortably. However, some patients with inadequate abdominal respiration did not improve.
DISCUSSION
In most cases, laryngeal granulomas are observed on the vocal process, but not on the vocal fold [5, 6]. Therefore, such cases generally have low grade hoarseness and subjective symptoms. In our experience, in 9 of 29 cases with laryngeal granulomas the chief complaint was hoarseness. Some researchers [7, 8] have insisted that gastroesophageal reflux disease (GERD) is an increasingly important factor in laryngeal granulomas. Laryngeal granulomas have been treated by PPI as the main therapy [9] . However, it is known that not all cases can be completely improved by PPI alone [4,10]. None of our cases with laryngeal granulomas were completely improved by PPI treatment for 8 weeks. Murry [10] described that patients with the primary complaint of cough and laryngeal adductor reflex (LAR) following the diagnosis of paradoxical vocal fold movement (PVFM) exhibited improvement in the laryngeal sensation with an associated resolution of PVFM and chronic cough after treatment with PPI and training for abdominal respiration despite the persistence of cough when treated with PPI alone. The results of the present study suggest that the cough associated with PVFM could be attributed to the decreased mechano-sensitivity resulting from receptors buried in the edematous mucosa. This is a hallmark of LPR and can be expected to improve with treatment. In those with PVFM, although the PPI might reduce the edema, the behavioral response (cough) required further treatment with behavioral methods, namely respiratory retraining. Decreased mechanosensitivity and chemosensitivity of the laryngopharyngeal mucosa from chronic acid irritation results in the increased collection of particulate or irritants in the laryngopharyngeal mucosa, and the chronic cough reflex might be simply an adaptive mechanism that has evolved through habit to clear the larynx. The paradoxical adduction of the vocal folds during inspiration in this context might serve as a protective response to prevent further inhalation of particulate matter in patients whose cough is not controlled by pharmacological treatment alone. Hyperfunctional dysphonia as well as GRAD and chronic cough are thought to cause laryngeal granuloma. [2, 11]
Those of our cases in which the symptoms disappeared had hyper-functional dysphonia at the first medical examination but improved using our method of voice training. In our study, the causes of the laryngeal granulomas in each case could not be determined whether among GRAD, chronic cough or hyperfunctional dysphonia. In the therapy for laryngeal granulomas, surgery is less effective than PPI treatment. Some researchers [4, 12-14] have reported high rates of postoperative recurrence (approximately 50-90%). Hyodo [4] in Japan reported that the effective rate of PPI was 42% (11/26). Nevertheless, our cases of laryngeal granulomas with resistance to proton pump inhibitor (PPI) without other therapies (e.g, silent therapy, medicine, operation) showed an effective rate of 89.6% (26/29), demonstrating disappearance or reduction by our method of voice training. In 4 cases with postoperative recurrence that was not improved by PPI treatment, the laryngeal granulomas disappeared after using only our voice training method.
The above mentioned reports and our results suggest that our method of voice training, by emphasizing the importance of abdominal respiration, might be useful for laryngeal granulomas due to chronic cough with GRAD and hyperfunctional dysphonia. Our study did not examine the physiological or aerodynamic mechanisms by which this voice training method caused the disappearance of the laryngeal granulations. All patients were able to speak comfortably after mastering abdominal respiration possibly because abdominal respiration contributed to relaxing the vocal fold resulting in the disappearance or reduction of the laryngeal granulations. Recently, Eherer [15] reported that abdominal breathing exercise could be positively effect for GERD by actively training the crura of the diaphragm as part of the lower esophageal sphincter. And he recommended this non-pharmacological lifestyle intervention could help to reduce the disease burden of GERD.
AUTHOR'S CONTRIBUTIONS
Kusunoki T. was involved in all staged of the study and were involved in date collection. Ikeda K. contributed to improving the manuscript. All authors read and approved the final manuscript.
ACKNOWLEDGEMENTS
This study is carried out at our institute thank to my teachers seniors and colleague who help to make this very rare case report.
REFERENCES
- Niimi S. (2011). Vocal rehabilitation. J Jpn Brochoesophagol Soc. 62: 433-439.
- Japan ORLSo. Oto-rhino-laryngological dictionary, vol. 1, 1 edn: Kyoto,Kinpodo. 2010.
- Kusunoki T, Monju and Ikeda K. (2013). Effectiveness of a simple voice training method by placing great importance on abdominal type of respiration. Pract Otol (Kyoto). 137: 124-125.
- Hyodo M, Taguchi A and Kobayashi J. (2004). The Larynx Japan. 16: 102-105.
- Cherry J and Margulies SI. (1968). Contact ulcer of the larynx. The Laryngoscope. 78(11): 1937-1940.
- Oda M. (1985). Investigations of pathogenesis of postintubation laryngeal granulomas. Otologica Fukuoka. 31: 295-314.
- Delahunty JE and Cherry J. Experimentally produced vocal cord granulomas. The Laryngoscope. 1968. 78(11): 1941- 1947.
- Jackson C and Jackson C. Contact ulcer of the larynx. Archives of otolaryngology. 1935. 22(1): 1-15.
- Wani MK and Woodson GE. (1999). Laryngeal contact granuloma. The Laryngoscope. 109(10): 1589-1593.
- Murry T, Branski RC, Yu K, Cukier-Blaj S, et al. (2010). Laryngeal sensory deficits in patients with chronic cough and paradoxical vocal fold movement disorder. The Laryngoscope. 120(8): 1576-1581.
- Feder RJ and Michell MJ. (1984). Hyperfunctional, hyperacidic, and intubation granulomas. Archives of otolaryngology. 110(9): 582-584.
- Havas TE, Lacst JP and Lowinger DSG. (1999). A management strategy for vocal process granulomas. Laryngoscope.109: 301-306.
- Tachibana T, Orita Y, Makino T, Ogawara Y, et al. (2016). A clinical study on 64 cases of laryngeal granuloma. Nippon Jibiinko Gakkai Kaiho (Tokyo). 119: 860-866.
- Ylitalo R and Lindestad PA. (1999). A retrospective study of contact granuloma. Laryngoscope. 109(3): 433-436.
- Eherer AJ, Netolitzky F, Hogenauer C, Puschnig G, et al. (2012). Positive effect of abdominal breathing exercise on gastro-esophageal reflux disease: a randomized. Controlled study. AM J Gastroenterol. 107(3): 372-378.