Previous Issues Volume 2, Issue 1 - 2017
Characteristics and Outcomes of Delayed Open Globe Repair
Sebastian P. Lesniak1, 2,Xintong Li2 ,Alain Bauza2 ,Nishant Soni2 ,Marco A. Zarbin2 ,Paul Langer2 ,Neelakshi Bhagat2*
1Matossian Eye Associates, Hopewell, NJ, USA.
2Rutgers New Jersey Medical School, Newark, NJ, USA.
Corresponding Author: Bhagat N. Department of Ophthalmology, Rutgers New Jersey Medical School, Doctors Office Center, Suite 6100, 90 Bergen Street, Newark, New Jersey, 07103, USA, Tel: 973-972-2032;
E-Mail: [email protected]
Received Date: 01 Feb 2017 Accepted Date: 09 Feb 2017 Published Date: 14 Feb 2017
Copyright © 2017 Bhagat
Citation: Bhagat N, Li X, Bauza A, Lesniak SP, et al. (2017). Characteristics and Outcomes of Delayed Open Globe Repair. Mathews J Ophthalmol. 2(1): 013.
ABSTRACT
Background: The purpose of this study is to evaluate the demographics, characteristics, and outcomes of delayed open globe repair. Methods: Retrospective chart review of patients with = 3 days between injury to globe repair that presented to our institution from 2001-2010. Results: Thirty-six patients with delayed open globe repair were identified; mean delay was 6.3 days (range: 3-21) and was due to delay by patient in seeking treatment (61%), outside referral (31%), unstable medical condition for surgery (6%), and Patient’s initial refusal of surgery (3%). There were 26 accidental injuries, 5 violent assaults, 2 motor vehicle accidents, 2 unspecified injuries, and 1 wound dehiscence. Eighteen injuries were penetrating, 15 were ruptures, and 3 were intraocular foreign bodies (IOFB). All 3 cases of endophthalmitis (8.3%, 1 with IOFB) were diagnosed upon admission for open globe injury; mean duration from injury to surgery was 5.7 days. Eight patients (22.2%) had retinal detachments and underwent pars-plana vitrectomy; five (62.5%) had complete retinal attachment at last follow-up. Mean presenting initial visual acuity was 1.67 logMAR (Snellen:20/929); mean final corrected visual acuity was 1.21 logMAR (Snellen:20/327). Conclusions: We noted endophthalmitis in 8.33% of eyes with delayed surgical repair by = 3 days. Timely and accurate diagnosis with appropriate referral for surgical intervention may decrease risk of endophthalmitis.
KEYWORDS
Open Globe Injury; Endophthalmitis; Eye Trauma; Delayed Repair; Visual Acuity.
INTRODUCTION
Open globe injury is a full-thickness wound of the eyewall [1]. The four main types of open globe trauma defined by Pieramici et al include: penetration, perforation, intraocular foreign body (IOFB), and rupture [1]. It has reported that 2.4 million eye injuries occur in the United States each year [5, 6, 8-10]. Open globe injuries may cause significant and irreversible damage to intraocular structures [4]. These injuries are the major cause of visual loss in urban populations, as well as the most common cause of monocular blindness [2, 4-6, 10]. The visual prognosis in eyes with open globe injury is often poor and depends on a number of factors such as the location and extent of the injury, and the presence of infection. Delay of primary open globe repair may be a risk factor for endophthalmitis [11, 12]. Other risk factors for endophthalmitis after trauma include IOFB, lens rupture, rural trauma, and trauma with contaminated objects [11]. The incidence of endophthalmitis following open globe trauma ranges from 3.1% to 11.9% of open globe injuries in the absence of an IOFB, while the incidence in cases with an IOFB ranges from 3.8% to 48.1% [11]. Primary repair of open globe injury should be performed preferably within 24 hours as a protective measure against endophthalmitis [14-16]. The purpose of this study is to evaluate the epidemiology, characteristics, and outcomes of open globe injuries which underwent repair delayed by 3 days or more after injury.
SUBJECTS AND METHODS
Approval from the Institutional Review Board at New Jersey Medical School, Newark, was obtained to conduct a retrospective chart review of patients who presented with open globe injuries to University Hospital, Newark, between January 2001 and December 2010 and underwent primary open globe repair 3 or more days after the initial injury. The data recorded from the patient charts included: age, race, gender, mechanism of injury, trauma classification (penetration, perforation, rupture, IOFB), time from injury to first surgery, reason for delay, additional surgeries performed, culture results, and intravenous (IV) antibiotics used. Ocular examination variables included were: initial and final visual acuity (VA), presence of an afferent pupillary defect (APD), zone of injury, lens status, retinal detachment (RD), vitreous haemorrhage (VH), endophthalmitis, and sympathetic ophthalmia (SO). The VA was converted from Snellen acuity to logMAR for the purpose of calculations. VA not reported in Snellen units was converted to logMAR as follows: counting fingers (CF)=1.6, hand movements (HM)=2.0, light perception (LP)=2.5, and NLP=3.0 logMAR units [17]. The zone of injury was classified according to the system described by Pieramici et al. [1] Zone 1 was defined by injury limited to the cornea, zone 2 by injury which extended up to 5 mm posterior to the limbus, and zone 3 by injury which extended more than 5 mm posterior to the limbus [1].
RESULTS
Thirty-six eyes (5.28%) with open globe injuries had delayed repair of 3 or more days out of 682 total open globe injuries that presented to University Hospital between 2001 and 2010. The demographic information is presented in Table 1. The mean age was 39.6 years and the majority of patients were male (67%).
Table 1: Clinical Characteristics of Eyes with Delayed Open Globe Repair.
| Age in years | |
|---|---|
| Mean | 39.6 |
| Range (min, max) | (1, 86) |
| Gender [# (%)] | |
| Males | 24 (67%) |
| Females | 12 (33%) |
| Race [# (%)] | |
| African American | 9 (25%) |
| Caucasian | 5 (14%) |
| Hispanic | 3 (8%) |
| Other/not defined | 19 (53%) |
The ocular trauma score (OTS) is calculated based on presenting VA, and the presence of any of the following: afferent pupillary defect, rupture injury, retinal detachment, endophthalmitis, and perforating injury [8]. OTS could only be calculated in 13 out of 36 cases (36.1%) due to missing variables in the medical records. Four patients received a score of 1, 3 a score of 2, 5 a score of 3, 0 a score of 4, and 1 a score of 5. The characteristics of the injuries are presented in Table 2. The most common injury classification was penetration (50%) closely followed by rupture (42%). IOFB represented 8% of cases. Zone 1 or corneal laceration, was the most common zone of injury (55%), and the most common causes of injury were accidents (72%).
Table 2: Injury Characteristics of Eyes with Delayed Open Globe Repair.
| Classification of injury [# (%)] | |
|---|---|
| Penetration | 18 (50%) |
| Rupture | 15 (42%) |
| Intraocular foreign body | 3 (8%) |
| Zone of injury [# (%)] | |
| 1 (Corneal) | 20 (55%) |
| 2 (Up to 5 mm posterior to the limbus) | 6 (17%) |
| 3 (Beyond 5 mm posterior to the limbus) | 9 (25%) |
| Unknown | 1 (3%) |
| Causes of injury [# (%)] | |
| Accident | 26 (72%) |
| Violence | 5 (14%) |
| Motor vehicle accident | 2 (5%) |
| Other | 2 (5%) |
| Wound dehiscence | 1 (3%) |
| Complications [# (%)] | |
| Retinal detachment | 8 (22%) |
| Endophthalmitis | 3 (8%) |
The time from injury date to open globe repair surgery is presented in Figure 1, and the mean duration of delay was 6.3 days (range, 3-21). The most common reasons for delay were a delay in seeking treatment by the patient (61%), and a delay in referral from an outside facility (31%) as presented in Table 3. Of note the patient whose repair was delayed by 21 days was referred from an outside institution.
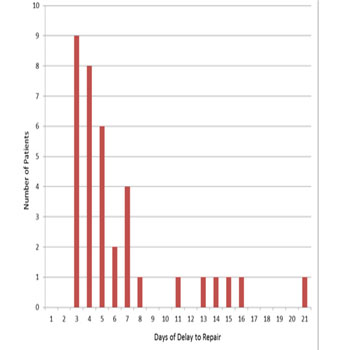
Figure 1: Days elapsed between injury and repair for eyes in this series. Table 3: Reasons for Delayed Open Globe Repair.
| Delay in seeking treatment by the patient | 22 (61%) |
| Outside referral | 11 (31%) |
| Unstable medical condition for surgery | 2 (6%) |
| Patient’s initial refusal to undergo surgery | 1 (3%) |
The average presenting initial visual acuity was 1.67 logMAR (Snellen 20/929), and the average final corrected visual acuity was 1.21 logMAR (Snellen 20/327). The acuities for each patient are presented in Figure 2. Thirteen patients (36.1%) presented with VA of HM or less.
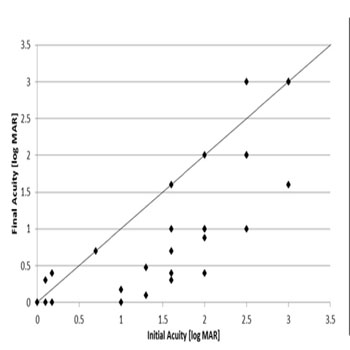
Figure 2: Visual acuity upon injury presentation and after repair.
Eight patients (22.2%) were diagnosed with retinal detachments, and 9 (25%) with choroidal detachments at presentation. All patients with retinal detachment underwent parsplana vitrectomy, 6 during primary repair. 6 were discharged home the same day, immediately after open globe repair, on oral systemic antibiotics and 2 underwent primary enucleations. The average length of stay in the hospital was 4.03 days (range 1-21 days). Twenty-eight patients (78%) received IV antibiotic therapy. The most common antibiotic combination was ceftazidime and vancomycin, followed by cefazolin and levofloxacin. Of the remaining 8 patients not on IV therapy, none of which developed endophthalmitis, 6 were discharged home the same day on oral systemic antibiotics and 2 underwent primary enucleations. Three (8.33%) of 36 eyes were diagnosed with endophthalmitis at presentation; all 3 cases were noted to have hypopyon and vitritis with an open globe. All 3 cases were zone 1 injuries. Uveal prolapse was not noted in any of these cases, and none of these wounds were reported to be contaminated. One patient was previously diagnosed with diabetes mellitus, while the other 2 patients had no past medical history or other evidence of immunocompromised status. The mean duration from injury to surgery for these 3 cases was 5.7 days. All underwent pars-plana vitrectomy (PPV) during primary open globe repair surgery, with injection of intravitreal antibiotics vancomycin (1mg/ 0.1 cc) and ceftazidime (2.25 mg/0.1 cc). All 3 patients were admitted for IV vancomycin and ceftazidime, with an average length of admission of 5 days (range 4-6 days) and were discharge on oral levofloxacin. Patients with endophthalmitis presented with initial acuity of CF, CF, LP, and their final acuities were 20/100, 20/200 and HM respectively. Metallic IOFB was diagnosed in 1 of these cases of endophthalmitis. The other patients were injured by glass bottle and light bulb fragments, but without IOFBs. The metallic IOFB was a projectile and the injury occurred while hammering at home. In this case vitreous cultures were negative. In the remaining 2 cases of endophthalmitis, the vitreous cultures grew methicillin-sensitive Staphylococcus aureus and Gemella (Streptococcus) morbillorum.
DISCUSSION
Delayed open globe repair cases represented 5.28% all cases of open globe injuries at our institution from 2001 to 2010. Delay in seeking treatment and outside referral were the most common reasons causing delay of primary open globe repair. This finding underscores the need for greater awareness of the seriousness of these injuries, and the need for prompt surgical management. Males represented a larger percentage of patients undergoing delayed repair, but this may reflect the overall higher prevalence of open globe injuries among males. The most common cause of injury was an accident, and the most common injury classification was penetrating injury. None of the injuries were associated with soil contamination. These characteristics are both consistent with many other previously published studies. Among the 3 cases of IOFB, only 1 developed endophthalmitis, and the object was a metallic projectile. The other 2 cases of IOFB, which did not result in endophthalmitis, involved a plant thorn and a piece of metal. Only the eyes diagnosed with endophthalmitis underwent intravitreal antibiotic injection. All patients were treated with systemic antibiotics; 6 were switched to oral therapy after one day of intravenous antibiotics; 28 patients (78%) received an average of 5 days of intravenous antibiotics before discharge. None of the eyes developed endophthalmitis once they underwent open globe repair. Endophthalmitis was noted in 8.33% of eyes in our study group that were repaired 3 or more days after the injury. All of these eyes had infection at presentation with open globe injury. This rate is comparable to the 6.8% published by Essex et al. [12]; Ahmed et al. [16] reported a rate upto 16.5%. In comparison, the total number of post-traumatic cases of endophthalmitis at our institution in the same period from 2001-2010 was 18 out of 682 total open globe injuries (2.64%). Thus, in the cohort with delayed surgical repair, the risk of endophthalmitis was more than 3 times higher. Essex et al. [12] concluded that a delay of as little as 12 hours is a statistically significant risk factor, while Ahmed et al. [16] reported that a delay of more than 24 hours increases the risk of endophthalmitis. In our 3 cases of endophthalmitis, the injuries were limited to the cornea, with the largest being a 6 mm laceration, and one eye had a metallic IOFB. The presence of a metallic IOFB is considered by many clinicians to be a risk factor for endophthalmitis. No uveal prolapse was noted in these cases, which can possibly increase the risk of endophthalmitis. All patients were phakic on presentation, and none had a retinal or choroidal detachment. In our study all 3 patients with endophthalmitis were diagnosed on presentation, and they all underwent PPV with intravitreal antibiotic injection. All 3 patients were admitted for IV antibiotic therapy and were subsequently discharged on oral antibiotics. In cases of delayed closure of open globe injury with IOFB even with no evidence of infection, one may consider intracameral antibiotics prophylactically [11, 16]. Use of prophylactic antibiotics is controversial due to lack of large randomized studies. Some authors report no decrease in risk of infection with prophylactic antibiotics, and argue against prophylaxis due to retinal toxicity and drug resistance [12, 14]. Except for the 2 cases of primary enucleation, none of the remaining cases required enucleation by the end of follow up period. Furthermore, the average final visual acuity achieved in our series of patients with endophthalmitis (1.233 log MAR or Snellen 20/342) was comparable to that of patients without endophthalmitis (1.212 logMAR or Snellen 20/326). The vitreous cultures grew methicillin-sensitive Staphylococcus aureus and Gemella (Streptococcus) morbillorum in the 2 culture-positive cases, and showed no growth in the third case. These culture results are consistent with prior published reports, which consistently report Staphylococcus and Streptococcus species as the most common causes of posttraumatic endophthalmitis [11, 14, 16]. The main limitations of this study stem from the difficulty in controlling many of the clinical variables associated with open globe injuries in a retrospective analysis. In many cases not all the variables were available from the charts as evidenced by the limited analysis of OTS that was possible. Visual prognosis in open globe injuries remains poor, even after prompt surgical intervention, Timely and accurate diagnosis, as well as appropriate referral for surgical intervention may decrease the risk of endophthalmitis.
REFERENCES
- Pieramici DJ, Sternberg P Jr, Aaberg TM Sr, Bridges WZ Jr, et al. (1997). A System for Classifying Mechanical Injuries of the Eye (Globe). Am J Ophthalmol. 123(6): 820-831.
- Kim JH, Yang SJ, Kim DS, Yoon YH, et al. (2007). FourteenYear Review of Open Globe Injuries in an Urban Korean Population. J Trauma. 62(3): 746-749.
- May DR, Kuhn FP, Morris RE, Mann L, et al. (2000). The Epidemiology of Serious Eye Injuries from the United States Eye Injury Registry. Graefes Arch Clin Exp Ophthalmol. 238(2): 153-157.
- Gupta A, Rahman I and Leatherbarrow B. (2009). Open Globe Injuries in Children: Factors Predictive of a Poor visual Acuity. Eye (Lond). 23(3): 621-625.
- Rahman I, Maino A, Devadason D and Leatherbarrow B. (2006). Open Globe Injuries: Factors Predictive of Poor Outcome. Eye (Lond). 20(12): 1336-1341.
- Salvin JH. (2007). Systematic Approach to Pediatric Ocular Trauma. Curr Opin Ophthalmol. 18(5): 366-372.
- Brophy M, Sinclair S, Hostetler G and Xiang H. (2006). Pediatric Eye Injury-Related Hospitalizations in the United States. Pediatrics. 117(6): e1263-e1271.
- Kuhn F, Maisiak R, Mann L and Witherspoon CD. (2002). The Ocular Trauma Score (OTS). Ophthalmol Clin North Am. 15(2): 163-165.
- Hill JR, Crawford BD, Lee H and Tawansy KA. (2006). Evaluation of Open Globe Injuries of Children in the Last 12 Years. Retina. 26(7 Suppl): S65-S68.
- Farr AK, Hairston RJ, Humayun MU, Juan E Jr et al. (2001). Open Globe Injuries in Children: A Retrospective Analysis. J Pediatr Ophthalmol Strabismus. 38(2): 72-77.
- Bhagat N, Nagori S and Zarbin M. (2011). Post-traumatic Infectious Endophthalmitis. Surv Ophthalmol. 56(3): 214-251.
- Essex RW, Yi Q, Charles PG and Allen PJ. (2004). Post-traumatic endophthalmitis. Ophthalmology. 111(11): 2015-2022.
- Danis RP. (2002). Endophthalmitis. Ophthalmol Clin North Am. 15(2): 243-248.
- Zhang Y, Zhang M, Jiang C and Zhang K. (2010). Endophthalmitis following open globe injury. Br J Ophthalmol. 94(1): 111-114.
- Thompson JT, Parver LM, Enger CL and Liggett PE. (1993). Infectious endophthalmitis after penetrating injuries with retained intraocular foreign bodies. National Eye Trauma System. Ophthalmology. 100(10): 1468-1474.
- Ahmed Y, Schimel AM, Pathengay A, Flynn HW Jr, et al. (2012). Endophthalmitis following open-globe injuries. Eye (Lond). 26(2): 212-217.
- Arroyo JG, Postel EA, Stone T, Egan KM, et al. (2003). A matched study of primary scleral buckle placement during repair of posterior segment open globe injuries. Br J Ophthalmol. 87(1): 75-78.