Previous Issues Volume 2, Issue 1 - 2017
Fetal Myocardial Infarction as Cause of Intrauterine Death
José Luis Gallo Vallejo1 *, Puerta Sanabria JM2 , López López N3
1Associate Professor at the University of Granada, Granada, Spain. 2Resident Physician, Obstetrics and Gynecology Service, University Hospital Virgen de las Nieves, University Hospital Complex of Granada, Granada, Spain. 3Resident Physician, Pathological Anatomy Service, University Hospital Virgen de las Nieves. University Hospital Complex of Granada, Granada, Spain. Corresponding Author: José Luis Gallo Vallejo, Head of Section, Obstetrics and Gynecology Service, University Hospital Virgen de las Nieves, University Hospital Complex of Granada, Associate Professor at the University of Granada, Granada, Spain, Tel: 34-657841361; Email: [email protected]
Received Date: 30 Jan 2017 Accepted Date: 14 Mar 2017 Published Date: 17 Mar 2017
Copyright © 2017 Vallejo JLG
Citation: Vallejo JLG, Sanabria JMP and López NL. (2017). Fetal Myocardial Infarction as Cause of Intrauterine Death. Mathews J Gynecol Obstet. 1(1): 007.
ABSTRACT
This paper describes the process by which fibrosis and calcification on the right ventricle papillary muscle –lesions associated with evolved myocardial infarction (MI)–was identified as the ultimate cause of intrauterine fetal death (FD). This is the first case described of fetal MI as a determining cause of FD in utero, with no malformative pathology or tumor present. Just a case of early neonatal death from MI due to thrombotic occlusion of the left coronary artery was found, which suggests that the event could happened during childbirth or even in utero.
KEYWORDS
Myocardial Infarction; Fetal Death; Intrauterine Death.
INTRODUCTION
The consequences of fetal death (FD) involve, primarily, a great emotional impact that affects the woman giving birth, her partner, the attending physician, and the institution assisting the event. Causes of FD have traditionally been classified into three groups: maternal, fetal and placental. Myocardial Infarction (MI), however, has never been identified as one of the causes behind FD in utero. This paper presents a case where fibrosis and calcification on the right ventricle papillary muscle –lesions directly associated with evolved MI–, were identified as the ultimate cause of intrauterine FD.
CASE REPORT
40 years old pregnant patient, P1011. Family records include father with heart disease, but no traces of coagulopathies, hypercholesterolemia or MI. She did not have any pathology or receive any added treatment. Pregnancy proceeds normally, with the last ultrasound conducted on week 32, and no abnormal findings. She did not undergo any infectious process during this time. The patient comes into the emergency room on week 33+6, reporting the absence of fetal movement during the 48 hours preceding hospital admission. The patient did not report hydrorrhea or bleeding. First examination reveals the existence of a uterine height smaller than amenorrhea, but with normal uterine tone. Cervix was closed and formed, and the fetus was in cephalic presentation. The abdominal ultrasound confirms the existence of a dead fetus, placenta on high front face and a severe oligoamnios. Blood test results were normal. Labor was induced with prostaglandins, thus ending it spontaneously. A male fetus was born with maceration signs. Fetus weighed 1800g, with Apgar score 0-0 and no apparent abnormalities. A histological study of the fetus and placenta was performed.
HISTOLOGICAL REPORT
Male fetus with sometometry corresponding to a gestation of 33-34 weeks somatometry. Renal maturation corresponding to about 30 to 31 weeks. Less than one week maceration. No malformations, infection or neoplasia. Fibrosis and calcification of right ventricle papillary muscle (Figures 1 and 2). Extramedullar hematopoiesis inside the heart. Hyperplastic bone marrow. Scarce remains of aspiration in the lung. Placental chorionic villi with aging and ischemia signs. Retroplacental bleeding with infarction areas. Final diagnosis: injuries identified in right ventricular papillary muscle would correspond to evolved MI. Medullary and extramedullary hematopoietic activity in the absence of signs of fetal distress (such us bleeding) suggests a case of anemia with unknown origin, which could be the cause of fetal MI.
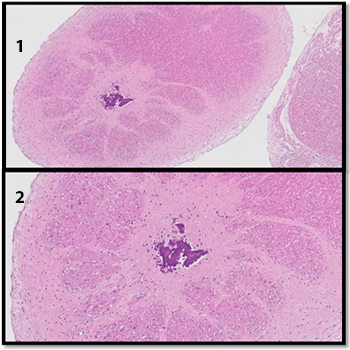
Figures 1 y 2: Fibrosis and calcification of right ventricle papillary muscle
DISCUSSION
No cases have been recorded in existing literature that identify fetal MI as the ultimate cause of fetal death in utero, particularly when no malformation or tumor had been previously identified. Literature exists, however, that describes how certain fetal cardiac tumors could cause fetal MI and intrauterine death due to their growth during pregnancy and subsequent compression of the coronary arteries [1]. Prenatal cardiac tumors, which represent 2.8% of cardiac disorders diagnosed in utero, have generally been classified into five types: rhabdomyoma, teratoma, atrial hemangioma, fibroma, and hamartoma. Rhabdomyoma is the most frequent of all, representing 86% of the total [2]. These tumors tend to increase their size as pregnancy progresses, due to the influence of maternal hormones. As a result, they may not be displayed in the prenatal ultrasound diagnosis at 20 weeks, and the vast majority appears at the end of the second or third quarter, or even in childhood [3]. There is a relatively small but yet significant association (11%) between cardiac tumors and spontaneous fetal loss, probably due to the compression of the coronary arteries, which can in turn lead to the appearance of MI and fetal death. This is the reason why a useful predictor of fetal cardiac tumors is, besides their number and size, the location of the tumor, as an obstruction to outflow of the right ventricle or an arrhythmia may determine fetal death in utero [4]. In the case described herein, no malformation or cardiac tumor was observed; only fibrosis and calcification of the right ventricle papillary muscle was identified. Also, the autopsy report revealed fetal anemia with unknown origin as the possible root cause of the fetal MI. Other cases of early neonatal death have been described in the past. Takeuchi et al [5].explains a case where death caused by fetal MI was due to thrombotic occlusion of the left coronary artery, which suggests the event could have occurred during labor. Muraskas et al [6]. describes an incident where the fetus had no signs of cardiac structural abnormality, and based on clinical, laboratory and autopsy data, concludes that MI could have occurred in utero. In closing, while previous cases of early neonatal death have been described, this is the first case reported of fetal death in utero as a result of fetal MI with no concomitant cardiac malformation or tumor pathology.
REFERENCES
- Sharma V and Sharma P. (2015). Peripartum onset of obsessive-
- Allan I. Fetal cardiac tumors. In: Allan I, Hornberger I, Sharland G. (2000). Textbook of fetal cardiology. London: Greenwich Medical Media limited. 358-365.
- Allan I. Fetal cardiac tumors. In: Allan I, Hornberger I, Sharland G. (2000). Textbook of fetal cardiology. London: Greenwich Medical Media limited. 358-365.
- Eguiluz I, Doblas PA, Barber MA, Robles L, et al. (2003). Diagnóstico prenatal de rabdomioma cardíaco fetal. Clin Invest Gin Obst. 30: 137-40.
- Takeuchi M, Suzuki T, Nakayama M, Kenmochi M, et al. (2006). Neonatal myocardial infarction due to thrombotic occlusion. J Matern Fetal Neonatal Med. 19: 121-123.
- Muraskas J, Besinger R, Bell T, DeLeon S, et al. (1997). Perinatal myocardial infarction in a newborn with a structurally normal heart. Am J Perinatol. 14: 93-97.