Previous Issues Volume 1, Issue 1 - 2016
Sucessful Treatment of Buschke-Löwenstein Tumor Combining Surgery and Glucan Therapy
Rososchansky J1, Borsari R1, Orsatti GM1, Freitas FM1, Fassoni AA1, Marcolino LD1, Ramos BRA2, Marques MEA2, Silva MG2
Bauru State Hospital, Bauru, São Paulo, Brazil. 2Department of Pathology, Botucatu Medical School, São Paulo State University, UNESP, Brazil. Corresponding Author:Joel Rososchansky, Bauru State Hospital, Bauru, São Paulo, Brazil, Tel: (014) 3815-6238; Email: [email protected]
Received Date: 19 Apr 2016 Accepted Date: 17 May 2016 Published Date: 02 Jun 2016
Copyright ©2016 Rososchansky J
Citation: Rososchansky J, Borsari R, Orsatti GM, Freitas FM, et al. (2016). Sucessful Treatment of Buschke-Löwenstein Tumor Combining Surgery and Glucan Therapy. Mathews J Gynecol Obstet. 1(1): 003.
ABSTRACT
Background: Buschke-Löwenstein tumor (BTL) is a giant condyloma acuminatum considered to be a putative precancerous lesion with a high recurrence rate after treatment. Case Presentation: We report a 31-year-old patient presenting with a giant condyloma acuminatum in the perineum and vulvar region. The tumor was removed by wide radical excision followed by plastic reconstruction. The patient did not develop local recurrence or distant metastasis as observed over the one-year follow up appointment. Conclusion: This is a case report concerning successful treatment of Buschke-Löwenstein tumor combining surgery and Glucan therapy with excellent functional and cosmetic results.
KEYWORDS
Buschke-LöwensteinTumor; Treatment; HPV-6.
INTRODUCTION
Giant condyloma acuminatum or Buschke-Löwenstein tumor (BTL) is a slow-growing, locally aggressive and disfiguring cauliflower-like tumor that typically affects the anogenital and perianal regions. BTL is a rare HPV-induced squamous cell carcinoma. It was first described in 1925 by Buschke-Löwenstein as a benign carcinoma-like condyloma acuminatum [1]. Despite being histologically classified as a non-malignant tumor, malignant transformation can occur in 40-60% of cases and the recurrence rate after treatment can be as high as 67% [2, 3]. We report the case of a 31-year-old female patient with a history of vulvar lesion.
CASE REPORT
A 31-year-old woman, two previous cesarean sections, first coitus at age 14 and 5 sexual partners during lifetime with non-compliance of condom use and no sexual partner at the time of the investigation presented with a giant condyloma acuminatum with concomitant bacterial infection. Physical examination showed exophytic tumor on the mons pubis, labia majora, labia minora, vaginal introitus, perineum and anus (Figure 1). The patient reported a small warty lesion in the vulvar region one year ago associated with difficulty in defecation and sexual intercourse. She did not report weight loss and she was afebrile and hemodynamically stable. The patient was screened for HIV, syphilis and hepatitis B and C infections and the results were nonreactive. Clinical and cytological evaluations of the cervix and vagina could not be performed by the time of admittance because of mechanical obstruction.

Figure 1: A) Exophytic, cauliflower-like verrucous tumor with irregular surface on the mons pubic, labia majora, labia minora, vaginal introitus, perineum and anus; B) Postoperative after extensive surgical excision; C) 10th postoperative day showing local infection and suture dehiscence; d) 75th postoperative Day showing second intention healing; E and F) Late postoperative showing full recovery (1 year).
Since most of the exophytic lesions have a pedicled base, surgical excision of the condyloma was performed by fusiform incision with a safety margin of 0.5 cm. The wound was sutured by approximation of wound margins (Figure 1) and the perineum was healed by second intention. During the surgery a pap smear was sampled and clinical evaluation was performed. There were no macroscopic lesions in the cervix or vagina. Postoperatively, the patient developed dehiscence of the skin suture with secondary bacterial infection. Intravenous antibiotic therapy administered included cefalotin, metronidazole and garamycin, along with local application of potassium permanganate and four daily bandages embedded with Dersane®. On postoperative day 15, the infection cleared and the patient was discharged but still had a partially granulated wound. Patient was followed up weekly for 3 months for evaluation and sub-cutaneous application of Glucan (B-1,3-D-Glicopiranose) for 20 weeks. A repeated screening test for HIV, syphilis and hepatitis B and C infections were negative and the Pap smear showed no abnormalities. Histological examination of the excised tissue revealed papillomatosis, acanthosis, hyperparakeratosis and keratinocytes with polymorphic nuclei, dense chromatin, perinuclear halo and keratohyalin granules (Figure 2).
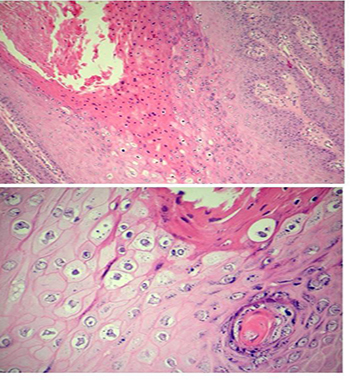
Figure 2: Hyperparakeratosis with polymorphic nuclei. papillomatosis and acanthosis. Keratinocytes with polymorphic nuclei, dense chromatin, perinuclear halo and keratohyalin granules.
The sample was screened for HPV DNA using the standard nested PCR approach of the MY09/11 primer set (primary PCR) and the GP5+/6+ primer set (secondary PCR) [4, 5]. The HPV genotype 6 was detected by multiplex PCR with consensus primers as described by Nishiwaki et al. [2]. The patient did not develop local recurrence or distant metastasis as observed over the one-year follow up appointment.
DISCUSSION
BTL is a rare sexually transmitted disease, triggered by HPV, especially by genotypes 6 and 11 [3, 6, 7]. The host immune response is involved in viral persistence and progression of lesions, and it has been suggested that the Buschke-Löwensteintumor might be an intermediate lesion within a continuous spectrum of biologically related tumors from the condyloma to the invasive squamous cell carcinoma [8]. This case demonstrates the classical findings of a Buschke-Löwenstein tumor regarding history, epidemiology and clinical features. BTL might occur at any age after puberty, usually between the 4th and the 6th decades and it can affect both men and women [9-12]. Risk factors include anoreceptive intercourse, HIV and immunosupression. Giant condyloma acuminatum affects glans penis, scrotum, vulva, perianal region and ano-rectum, with extremely rare involvement of the bladder although it has already been described [13]. Even though no standard treatment has been defined to BTL, most reports suggest that the radical surgical excision with resection of margins is the best choice if the anal canal is not involved [12]. Chemoradiation has also been used either in conjunction with radical surgery in cases of disease recurrence or as a sole treatment [14-16]. Another treatment employed is laser application and a recent report supports the use of oral acitrein and topical imiquimod in some cases [3, 17]. Patients with BTL must be very carefully investigated regarding the extension of penetration of the tumor into surrounding structures to ensure proper management of the lesion and the follow up is an essential part of the treatment as it allows the screening of relapse and malignization cases.
REFERENCES
- Buschke A and Löwenstein L. (1925). Über carcinomähnliche Condylomata acuminata des Penis. Klin Wochenschr. 4, 1726-1728.
- Nishiwaki M, Yamamoto T, Tone S, Murai T, et al. (2008). Genotyping of human papillomaviruses by a novel one-step typing method with multiplex PCR and clinical applications. J Clin Microbiol. 46(4), 1161-1168.
- Erek E, Basar H, Bozdogan O and Emeksiz MC. (2009). Giant condyloma acuminata of Buschke-Löwenstein: successful treatment with a combination of surgical excision, oral acitretin and topial imiquimod. Clin Exp. Dermatol. 34(3), 366-368.
- Manos MM, Ting Y, Wright DK, Lewis AJ, et al. (1989). Use of polymerase chain reaction ampli?cation for the detection of genital human papillomaviruses. Cancer Cells. 7, 209-214.
- De Roda Husman AM, Walboomers JMM, Van Den Brule AJC, Meijer CJLM, et al. (1995). The use of general primers GP5 and GP6 elongated at their 3’ends with adjacent highly conserved sequences improves human papillomavirus detection by PCR. J Gen Virol. 76, 1057-1062.
- Armstrong N, Foley G, Wilson J, Finan P, et al. (2009). Sucessful treatment of a large Buschke-Lowenstein tumor with chemo-radiotherapy. Int J STD & AIDS. 20(10), 732-734.
- Asato Y, Taira K, Yamamoto Y and Uezato H. (2008). Detection of human papillomavirus type 11 in a case of BuschkeLöwenstein tumor. Eur J Dermatol. 18(3), 329-331.
- Boshart M and zur Hausen H. (1986). Human Papillomaviruses in Buschke-Löwenstein Tumors: Physical State of the DNA and Identification of a Tandem Duplication in the Noncoding Region of a Papillomavirus 6 Subtype. J Virol. 58(3), 963-936.
- Skwronska-Piekarska U and Koscinski T. (2015). Buschke - Löewenstein tumor resection with simultaneous reconstruction of extensive tissue losses: case report. BMC Surg. 15, 41.
- Ambriz-Gonzáles G, Escobedo-Zavala LC, Carillo de la Mora F, Ortiz-Arriaga A, et al. (2005). Buschke- Löwenstein tumor in childhood: A case report. J Pediatr Surg. 40, e25-7.
- . De Toma G, Cavallaro G, Bitonti A, Polistena A, et al. (2006). Surgical management of perianal giant condyloma acuminatum (Buschke-Löwenstein tumor). Report of three cases. Eur Surg Res. 38(4), 418-422.
- Nthumba PT, Ngure P and Nyoro P. (2011). Giant condyloma acuminatum of the scrotum in a man with AIDS: a case report. J Med Case Reports. 5, 272.
- Wiedemann A, Diekmann WP, Holtmann G and Kracht H. (1995). Report of a case with Giant Condyloma Buschke-Löwenstein localized in the bladder. J Urology. 153(4), 1222-1224.
- Tytherleigh MG, Birtle AJ, Cohen CE, Glynne-Jones R, et al. (2006). Combined surgery and chemoradiation as a treatment for the Buschke-Löwenstein tumour. Surg J R Coll Surg. 4(6), 378-383.
- Dolanc R, Kocher T, Langer I, Marti WR, et al. (2002). Malignant transformation of perianal Buschke-Lwenstein tumor. Extensive abdominoperineal rectum excision and reconstruction with transpelvic myocutaneous rectus abdominis muscle flap. Chirurg. 73, 370-374.
- Sobrado CW, Mester M, Nadalin W, Nahas SC, et al. (2000). Radiation-induced total regression of a highly recurrent giant perianal condyloma: report of case. Dis Colon Rectum. 43, 257-260.
- Dias AS. (1994). Androscopy and treatment of human papillomavirus (HPV) with CO2 laser surgery. J Clin Laser Med Surg. 12, 277-280.