Previous Issues Volume 3, Issue 1 - 2018
Ideal Approach to Gastroesophageal Reflux in Pregnancy
Vedat Goral*
Corresponding Author: Vedat Goral, Department of Gastroenterology, Istanbul Medipol University Medical School Hospital, ISTANBUL, Turkey, Tel: 81-3-3480-1151 (3251); E-Mail: [email protected]
Received Date: 03 Jul 2018 Accepted Date: 31 Jul 2018 Copyright © 2018 Goral V
Citation: Goral V. (2018). Ideal Approach to Gastroesophageal Reflux in Pregnancy. Mathews J Gastroenterol Hepatol 3(1): 011.
ABSTRACT
Gastroesophageal reflux disease (GERD) in pregnancy is more common among women who become pregnant at an early age, suffered from reflux during previous pregnancies, have had reflux before pregnancy even though the extent of reflux had been limited, and had multiple pregnancies. GERD is multifactorial and is rare during the first trimester and after delivery. Progesterone plays a major role, whereas the involvement of mechanical factors is minor. Serious reflux complications are rare. Extra-esophageal symptoms (cough, hoarseness, precordial pain, laryngitis, tooth damage) do not become more frequent. GERD may have a prevalence of 45% and may be asymptomatic. GERD may occur only on some days. Regurgitation is more common than heartburn. GERD is 3.79 times more common during pregnancy in women who had GERD prior to pregnancy. GERD may be different in each pregnancy woman. Raft-forming-antireflux agents are safe and effective in GER treatment during pregnancy
INTRODUCTION
Gastroesophageal reflux (GER) is the passage of stomach's contents to the esophagus. Presence of structural changes in the esophagus and occurrence of symptoms affecting individuals' quality of life indicate gastroesophageal reflux disease (GERD) [1-6]. Gastroesophageal reflux develops in 30 to 50% of pregnant women but the incidence may be as high as 80% in some patient groups [1-4]. In Asian countries, the incidence varies between 2.5 to 7.5% [6]. Many studies indicate that the frequency of its symptoms increases from the first through the third trimester, resolving postpartum [3-5]. GERD tend to recur with subsequent pregnancies and affects multiparous and nulliparous women similarly. Pregnancy may precipitate or worsen GERD symptoms [7-9].
The root causes include decreased esophageal sphincter pressure due to the effects of the hormones, increased intraabdominal pressure due to enlarged uterus, prolonged passage of food from the intestine due to hormonal causes, and decreased lower esophageal tone. This high prevalence of reflux in pregnancy is due to both hormonal and mechanical causes. Manometer studies have demonstrated progressively declining basal lower esophageal sphincter (LES) pressure.
Increased progesterone hormone levels in pregnancy lead to more frequent and higher relaxation of the lower esophageal sphincter. Esophageal movements are also slowed down and gastric emptying time is prolonged. While this provides maximal food absorption for the developing fetus, the gastric pressure remains high and escape back is facilitated due to this effect. Enlarging fetus, hence the uterus, during the later phases of pregnancy lead to a gradual increase in intra-abdominal pressure, which produces pressure on the stomach, increasing reflux. Increased intra-abdominal pressure due to enlarged uterus is not considered to be adequate per se to provoke GER. A compensatory increase in LES pressure is observed in other conditions that elevate intra-abdominal pressure, such as abdominal ascites. This compensatory mechanism does not come into play in pregnancy. Sensitivity to acid contact in the esophagus may also be increased (hypersensitivity, sensitization), which is involved in reflux development. Studies in experimental animals have shown that estradiol lead to LES relaxation by impairing motility over potassium channels in the G protein-coupled estrogen receptor (GPER) [7].
GERD is multifactorial and is rare during the first trimester and after delivery. Progesterone plays a major role, whereas the involvement of mechanical factors is minor. Serious reflux complications are rare. Extra-esophageal symptoms (cough, hoarseness, precordial pain, laryngitis, tooth damage) do not become more frequent. GERD may have a prevalence of 45% and may be asymptomatic. GERD may occur only on some days. Regurgitation is more common than heartburn. GERD is 3.79 times more common during pregnancy in women who had GERD prior to pregnancy [8, 9].
Risk Factors Reflux in pregnancy is more common among women who become pregnant at an early age, suffered from reflux during previous pregnancies, have had reflux before pregnancy even though the extent of reflux had been limited, and had multiple pregnancies. Reflux in pregnancy is less common in advanced maternal ages. The frequency may decline with multiparity, gestational age and presence of reflux symptoms before pregnancy and advanced ages. GERD may be different in each pregnancy woman. Weight gain is a minor contributor [10]. Hormonal changes in pregnancy lead to relaxation of the LES muscle. Hormonal changes result in deceleration of esophageal motility and delayed descend of food to the stomach. Enlargement of the uterus during the second and third trimesters also lead to a gradually increasing pressure on the stomach by increasing intra-abdominal pressure. Some authors describe the role of this as a minor contribution. Reflux in pregnancy is frequent, but extra-esophageal complications are less common. Reflux symptoms diminish after delivery.
Diagnosis Presence of reflux is understood through patient's history. Upper gastrointestinal endoscopy is reliable and endoscopy is not risky in pregnancy. However, gastroenterologist still avoid this procedure in expectant mothers as far as possible. Endoscopy is indicated if reflux symptoms persist despite medical treatment and lifestyle changes or if additional symptoms including hematemesis or dysphagia are present. Manometer and pH-meter can be used safely but are seldom indicated.
TREATMENT
Diet and lifestyle changes Eating in 3-hour intervals and as small meals is important. Eating should also be slow and food should be thoroughly chewed. Water should not be drunk while eating and should be reserved to between meals, and all eating should be stopped 3 hours before bedtime. Chocolate, fatty/oily food, acidic drinks and food, caffeine, citrus fruits and tomato, ketchup and fizzy drinks should be avoided. Sitting up straight and walking slowly for one hour after meals provide relief. Individuals should wear comfortable clothes, maintain a healthy bodyweight, consume yoghurt or a glass of warm milk or chew sugar-free gums (increases salivation, thus neutralizing the acid that enters the esophagus) to suppress the symptoms. Food and drinks which are unlikely to increase reflux and are recommended include apples, bananas, baked potatoes, broccolis, cabbages, carrots, green beans, sweat peas, steak, chicken breast, egg whites, fish meat, cheese, goat cheese, bran, oat, corn bread, rice, mineral water, and oil-free salad [11, 12].
Individuals should drink chamomile tea or a glass of warm milk with some honey added, and should consult a physician for alternative medicine (e.g. yoga) treatments. Besides, raising bedhead or sleeping on the left side provides significant relief.
Medical Treatment Antacids or sucralfate should be used first. Symptomatic treatments without systemic effect or absorption should be preferred. Antacids, which are non-systemic drugs, should be initiated in pregnant women who do not respond to lifestyle changes, and they should be used as the first choice in treatment. They offer the required relief in many women with mild symptoms. Preferably, the antacid + alginic acid combination is more beneficial. Medicinal products containing antacid plus alginic acid act by forming a layer over the stomach content, neutralizing the existing acid and preventing the effect of the refluxing material on the esophageal mucosa (picture 1). It is recommended to take 15-30 ml of these products 15 minutes after meals and before bedtime. Suspension forms are particularly efficacious. Being affordable and readily available are the advantages of these medicines [13, 14].
Long-term and high-dose Mg++ trisilicate should be avoided, especially in the third trimester, as it may lead to contractions. Na+ bicarbonate should be avoided since it may lead to edema and hypertension. Those that contain aluminum may result in constipation.
Sucralfate As an aluminum salt that acts by inhibiting pepsin activity, sucralfate seems to be safe since it is not absorbed from the gastrointestinal tract [11,12]. Sucralfate is taken orally as 1 g three times daily but should this proves inadequate, it may be combined with lifestyle changes together with antacid + alginic acid treatment. No maternal or fetal side effects associated with sucralfate have been reported.
H2 receptor antagonist: Of the H2 receptor antagonists, ranitidine is FDA category B, while information on others is limited, and they may possibly be safe.
Differential Diagnosis Gallstones, stomach/esophageal cancer, peptic ulcer, esophageal motility disorders, drug-related esophagitis and eosinophilic esophagitis should be considered.
Prokinetic agents Data on their efficacy and safety in pregnancy is insufficient.
PPI The most efficient medical treatment choice in relieving reflux symptoms and treating esophagitis in the general population is currently the proton-pump inhibitors and they are commonly used. There are, however, some side effects associated with their long-term use. Omeprazole is a FDA category B drug, while information on others is limited, and they may possibly be safe [14-17].
Herbal methods: Ginger, chamomile, thymus, valerian, fenugreek, green tea, olibanum (oil derived from the sweetgum tree native to tropical zones) and quince sauce can be used. One study investigated quince sauce and ranitidine, and obtained comparable results [18].
In conclusion, gastroesophageal reflux in pregnancy is common but is well-managed with appropriate diet and medical treatment.
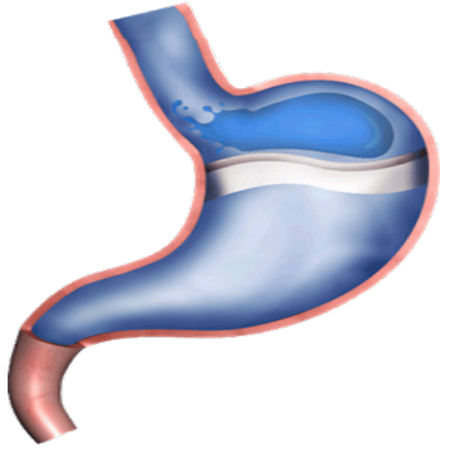
Figure 1: The acid pocket: A highly acidic fluid mass (average pH 1.6) that remains over the gastric content following a meal. This “pocket” is larger in reflux patients (diameter: 4-6 cm) [13,14]. Acid pockets form in the fundus following meals and reflux symptoms develop if escape occurs from here into the esophagus. It has been demonstrated in studies that alginate forms a layer on the fundus pocket and isolates the acid pocket from the esophagus.
REFERENCES
- Herregods TV, Bredenoord AJ and Smout AJ. (2015). Pathophysiology of gastroesophageal reflux disease: new understanding in a new era. NeurogastroenteroloMotil 27(9): 1202-1213.
- Ramya RS, Jayanthi N, Alexander PC, Vijaya S, et al. (2014). Gastroesophageal reflux disease in pregnancy: a longitudinal study. Trop Gastroenterol. 35(3): 168-172.
- Ramu B, Mohan P, Rajasekaran MS and Jayanthi V. (2011). Prevalence and risk factors for gastroesophageal reflux in pregnancy. Indian J Gastroenterol. 30(3): 144-147.
- Heidelbaugh JJ. (2018). Gastroesophageal Reflux Disease (GERD). Ambulatory Clinical Guidelines Oversight. 1-12.
- Bor S, Kitapcioglu G, Dettmar P and Baxter T. (2007). Association of heartburn during pregnancy with the risk of gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 5(9): 1035-1039.
- Wu JC. (2008). Gastroesophageal reflux disease: an Asian perspective. JGastroenterol Hepatol. 23(12): 785-1793.
- Tsai CC, Tey SL, Chang LC, Su YT, et al. (2018). Estradiol mediates relaxation of porcine lower esophageal sphincter. Steroids. 136: 56-62
- Rey E, Rodriguez-Artalejo F, Herraiz MA, Sanchez P, et al. (2018). Gastroesophageal reflux symptoms during and after pregnancy: a longitudinal study. Am J Gastroenterol. 102(11): 2395-2400.
- Malferttheiner SF, Malfertheiner MV, Kropf S, Costa SD, et al. (2012). A prospective longitudinal cohort study: evolution of GERD symptoms during the course of pregnancy. BMC Gastroenterol. 12: 131.
- Turan I, Kitapcioglu G, Tavmergen Goker E, Sahin G, et al. (2016). In vitro fertilization-induced pregnancies predispose to gastroesophageal reflux disease. United European Gastroenterol J. 4(2): 221-228.
- MacFarlane B. (2018). Management of gastroesophageal reflux disease in adults: a pharmacist's perspective. Integr Pharm Res Pract. 7: 41-52.
- Van der Woude CJ, Metselaar HJ and Danese S. (2014). Management of gastrointestinal and liver diseases during pregnancy. 63(6): 1014-1023.
- Quartarone G. (2013). Gastroesophageal reflux in pregnancy: a systematic review on the benefit of raft forming agents. Minerva Ginecol. 65(5): 541-549.
- Tygat GN, McColl K, Tack J, Holtmann G, et al. (2008). New algorithm for the treatment of gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 27(3): 249-256.
- Majithia R and Johnson DA. (2012). Are proton pump inhibitors safe during pregnancy and lactation? Evidence to date. Drugs. 72(2): 171-179.
- Matok I, Levy A, Wiznitzer A, Uziel E, et al. (2012). The safety of fetal exposure to proton-pump inhibitors during pregnancy. Dig Dis Sci. 57(3): 699-705.
- . Fill Malfertheiner S, Malfertheiner MV Mönkemüller K, , Röhl FW, et al. (2009). Gastroesophageal reflux disease and management in advanced pregnancy: a prospective survey. Digestion. 79(2): 115-120.
- Afsaneh Shakeri, Hashempur MH, Mojiban M, Aliasl F, et al. (2018). A comparative study of ranitidine and quince (Cydonia oblonga mill) sauce on gastroesophageal reflux disease (GERD) in pregnancy: a randomised, open-label, active-controlled clinical trial. J Obstet Gynaecol. 19: 1-7.