Previous Issues Volume 2, Issue 2 - 2017
Patients who Die Within Emergency Department: A Descriptive Study
1Tayfun Borta, 1 Umut Gulacti, 1 Ugur Lok, 1 Irfan Aydin, 1Ibrahim Halil Cebe, 1Ebru Arslan
1Department of Emergency Medicine, Adiyaman University Medical Faculty, Adiyaman-Turkey.
Corresponding Author: Umut Gulacti, Assistant Prof. Adiyaman University Medical Faculty, Department of Emergency Medicine, Adiyaman, Turkey, Tel: +90(535) 585 1900; E-Mail: [email protected]
Received Date: 15 May 2017 Accepted Date: 31 Jul 2017 Published Date: 02 Aug 2017
Copyright © 2017 Gulacti U
Citation: Borta T, Gulacti U, Lok U, Aydin I, et al. (2017). Patients who Die Within Emergency Department: A Descriptive Study. Mathews J Emergency Med. 2(2): 026.
ABSTRACT
Objectives: The characteristics of patients who die within the Emergency Department (ED) are important in describing its demographics. This study aimed to investigate the demographic and clinical characteristics of patients who died in one particular ED.
Method: This retrospective cross-sectional study was conducted between 01 January 2013 and 31 December 2015 at the Adiyaman University Training and Research Hospital, Turkey. Data were collected from the hospital medical records of all patients who died in the ED. Those aged 50 years and above were then divided into three groups: 50±64 years, 65±74 years, and 75 years and over.
Objectives: The characteristics of patients who die within the Emergency Department (ED) are important in describing its demographics. This study aimed to investigate the demographic and clinical characteristics of patients who died in one particular ED.
Results: A total of 355 patients who died within the ED were included in study. Their mean age was 57.8 ± 20.5 years (range: 0-114 years), and 53.8% were male. The most common primary complaint was chest pain. Of the patients, most (65.1%) died of cardiac diseases, followed by diseases of the respiratory system (13.5%), and cerebrovascular diseases (4.5%). The most frequent cause of ED deaths was acute myocardial infarction (MI) (n = 202, 56.6%). The highest mortality rate occurred in patients aged at least 50 years (n = 314, 88.5%). In the three distinct groups of patients aged at least 50 years, the highest mortality rate was observed in those aged 75 years and over (n = 156, 44%). Deaths caused by cardiac diseases were the most prevalent in the patients aged 71-80 years, while deaths caused by diseases of the respiratory and cerebrovascular systems were the most prevalent in the patients aged 81-114 years. A total of 58.8% of the patients had at least one chronic disease in their medical history. Recording of the major complaint was incomplete in 70.4% of patients. Conclusions: The highest mortality rate occurred in patients aged at least 50 years, and reached a maximum in those aged 75 years and over. The majority of the deaths within the ED were due to cardiovascular system diseases, and the most common diagnosis was acute MI. Deaths in the ED can be very traumatic for physicians, our study reinforces that the most common causes of death are in line with national statistics.
INTRODUCTION
The characteristics of patients who die are an outcome that can be used to improve knowledge of a service. Deaths in the emergency department (ED) have unique characteristics, and a description of deaths in the ED could be used to assess trends within individual institutions [1,2]. With an increasing number of patient admissions, the ED can become crowded and chaotic, and deaths are stressful situations that commonly occur in the routine work of an emergency physician. The high frequency of ED deaths necessitates that ED physicians prepare themselves for the issues surrounding death [1], and mortality statistics are important in the description of an ED [2]. Published studies describing patients who have died within the ED are scarce. This, and the fact that the ED patient databases cannot be fully developed, constitutes a great obstacle in determining ED requirements, and in revealing patient profiles [1, 2]. The present study aimed to investigate the demographic and etiologic characteristics of the patients who died in one particular ED.
MATERIALS AND METHOD
Study design and settings This retrospective, cross-sectional study was conducted in patients who died in the ED of Adiyaman University Training and Research Hospital between 01 January 2013 and 31 December 2015. It is a single center serving Adiyaman city, which is located in the west of the Southeastern Anatolia region of Turkey. There is no admission for pediatric patients in the Adiyaman University Training and Research Hospital ED, except for those requiring surgery.
The study was performed in compliance with the World Medical Association Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects and was approved by the Medical Ethics Committee (number: 1-11/2016). It was verified according to the checklist for observational studies in Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) and registered to Clinicaltrials (clinicaltrials.gov ID: NCT03138707).
Study population Data were collected from hospital medical records and patient ED charts, including demographic characteristics, major complaint, ED diagnosis, cause of death, and chronic diseases of patients. Patients who died in the ED and who arrived in cardiac arrest were included in study while patients missing ED charts were excluded. In order to identify the presenting complaint and diagnosis, an International Classification of Diseases (ICD) 10 code was used. The main diseases were classified into the following groups, according to organ systems: diseases of the cardiovascular system, diseases of the respiratory system, cancers, and "other system disease" for diseases with causes other than cardiac disease, respiratory system disease, cerebrovascular disease, and cancers. Patients aged 50 years and above were divided into three groups: 50±64 years, 65±74 years, and 75 years and over.
Outcome measures The primary outcome measure was the demographic characteristicsof the patients who died in the ED. The secondary outcome measure was the etiologic characteristics of the patients who died in the ED.
Statistical analysis The data were analyzed using SPSS (Statistical Package for the Social Sciences) software version 16.0. Numerical variables are expressed as mean ± standard deviation (SD), and categorical variables are expressed as number and percentage. Categorical variables were compared using the Chi-square test. Statistical significance was defined as p < 0.05.
RESULTS
A total of 358 patients died within the ED during the study period, but three patients could not be evaluated because their ED charts were missing. Ultimately, 355 patients were included in study. Deaths within the ED accounted for 0.0002% of patients who presented during the study period (355/1,520,000).
The mean age of the patients who died was 57.8 ± 20.5 years (range: 0-114 years), and 53.8% (n = 191) of the patients were male, while 46.2% (n = 164) were female. In distribution of deaths by age, the highest mortality rate occurred in patients aged 50 years and over (n = 314, 88.5%) (Figure 1).
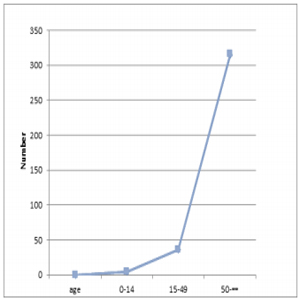
Figure 1: Distribution of patients who died within Emergency Department according to age.
When the patients aged 50 years and over were divided into three groups, the highest mortality rate was found in those aged 75 years and over (n = 156, 44%), followed by the 65- 74 age group with 24.8%, and the 50-64 age group with 20% (Figure 2).
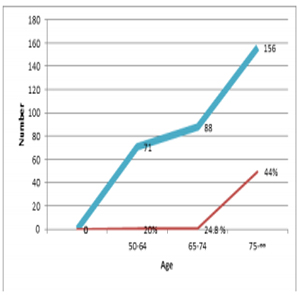
Figure 2: Distribution of patients aged 50 years and over.
The most frequent cause of death in the ED was acute myocardial infarction (MI) (n = 202, 56.6%), followed by cerebrovascular disease (n = 13, 3.6%) and aspiration pneumonia (n = 12, 3.4%). Causes of death of the patients are shown in table 1.
Table 1: Causes of Death
ARDS:Acute respiratory distress syndrome, HHNS: hyperglycemic hyperosmolar nonketotic syndrome, COPD: Chronic obstructive pulmonary disease
| Diseases | N | % |
|---|---|---|
| Acute myocardial infarction | 202 | 56.9 |
| Cerebrovascular disease | 13 | 3.6 |
| Aspiration pneumonia | 12 | 3.4 |
| Pulmonary edema | 11 | 3.1 |
| Ischemic heart disease | 11 | 3.1 |
| Pulmonary embolism | 10 | 2.8 |
| Sepsis | 7 | 1.9 |
| Heart failure | 7 | 1.9 |
| Cardiogenic shock | 6 | 1.7 |
| Sudden cardiac death | 6 | 1.7 |
| Pneumonia | 6 | 1.7 |
| Gastrointestinal bleeding | 6 | 1.7 |
| Mix type acidosis | 6 | 1.4 |
| Ventricular fibrillation | 5 | 1.7 |
| Traffic accident | 5 | 1.4 |
| Chronic renal failure | 5 | 1.1 |
| Acute respiratory failure | 4 | 1.1 |
| ARDS | 4 | 1.1 |
| Multiple organ insufficiency | 4 | 1.1 |
| Foreign body aspiration | 3 | 1.1 |
| Lung cancer | 3 | 0.8 |
| Brain edema | 3 | 0.6 |
| Respiratory arrest | 2 | 0.6 |
| HHNS | 1 | 0.3 |
| Gastric perforation | 1 | 0.3 |
| Acute renal failure | 1 | 0.3 |
| Pneumothorax | 1 | 0.3 |
| Anaphylaxis | 1 | 0.3 |
| Hypoglycemia | 1 | 0.3 |
| Alzheimer | 1 | 0.3 |
| Chronic lymphocytic leukemia | 1 | 0.3 |
| Chordoma | 1 | 0.3 |
| Anaphylaxis | 1 | 0.3 |
| Liver failure | 1 | 0.3 |
| COPD | 1 | 0.3 |
| Larynx cancer | 1 | 0.3 |
| Malignant neoplasm of liver | 1 | 0.3 |
| Malignant neoplasm of brain | 1 | 0.3 |
| Hypovolemic shock | 1 | 0.3 |
| Carbon monoxide poisoning | 1 | 0.3 |
When the main diseases were classified according to organ systems, the majority of deaths that occurred (65.1%, n = 231) were due to cardiovascular system diseases, followed by diseases of the respiratory system (13.5%, n = 48), cerebrovascular system diseases (4.5%, n = 16), other system diseases (12.4%, n = 44), cancers (2.8%, n = 10), and trauma (1.7%, n = 6) (p < 0.05)
When considering the distribution of organ system diseases caused by death according to age, Diseases of the cardiovascular system were the most prevalent in patients aged 71-80 years. Diseases of the respiratory and cerebrovascular system were the most prevalent in patients aged 81±114 years (Table 2).
Table 2: Distribution of organ system diseases caused by death according to age
| Age groups | Diseases | N | % |
|---|---|---|---|
| 0-10 years | |||
| Cardiac disease | 0 | 0 | |
| Respiratory System Disease | 4 | 80 | |
| Cerebrovascular Disease | 0 | 0 | |
| Other | 0 | 0 | |
| Cancers | 1 | 20 | |
| Total | 5 | 100 | |
| 11-20 years | |||
| Cardiac disease | 1 | 100 | |
| Respiratory System Disease | 0 | 0 | |
| Cerebrovascular Disease | 0 | 0 | |
| Other | 0 | 0 | |
| Cancers | 0 | 0 | |
| Total | 1 | 100 | |
| 21-30 years | |||
| Cardiac disease | 2 | 50 | |
| Respiratory System Disease | 1 | 25 | |
| Cerebrovascular Disease | 0 | 0 | |
| Other | 0 | 0 | |
| Cancers | 1 | 25 | |
| Total | 4 | 100 | |
| 31-40 years | |||
| Cardiac disease | 4 | 33.3 | |
| Respiratory System Disease | 4 | 33.3 | |
| Cerebrovascular Disease | 0 | 0 | |
| Other | 1 | 8.3 | |
| Cancers | 3 | 25 | |
| Total | 12 | 100 | |
| 41-50 years | |||
| Cardiac disease | 15 | 68.2 | |
| Respiratory System Disease | 1 | 4.5 | |
| Cerebrovascular Disease | 0 | 0 | |
| Other | 2 | 9 | |
| Cancers | 4 | 18 | |
| Total | 22 | 100 | |
| 51-60 years | |||
| Cardiac disease | 34 | 80.9 | |
| Respiratory System Disease | 4 | 9.5 | |
| Cerebrovascular Disease | 1 | 2.4 | |
| Other | 1 | 2.4 | |
| Cancers | 2 | 4.8 | |
| Total | 42 | 100 | |
| 61-70 years | |||
| Cardiac disease | 50 | 72.5 | |
| Respiratory System Disease | 7 | 10.1 | |
| Cerebrovascular Disease | 4 | 5.8 | |
| Other | 2 | 2.9 | |
| Cancers | 6 | 8.9 | |
| Total | 69 | 100 | |
| 71-80 years | |||
| Cardiac disease | 71 | 63.9 | |
| Respiratory System Disease | 17 | 15.3 | |
| Cerebrovascular Disease | 4 | 3.6 | |
| Other | 3 | 2.7 | |
| Cancers | 16 | 14.4 | |
| Total | 111 | 100 | |
| 81-114 years | |||
| Cardiac disease | 57 | 63.3 | |
| Respiratory System Disease | 19 | 21.1 | |
| Cerebrovascular Disease | 6 | 6.7 | |
| Other | 1 | 1.1 | |
| Cancers | 7 | 7.8 | |
| Total | 90 | 100 |
When examining the past medical history of the patients, 58.8% (n = 210) had at least one chronic disease, 23.5% (n = 84) had two chronic diseases, and 7.3% (n = 26) had three chronic diseases. The most common chronic diseases found in the medical histories were congestive heart failure and coronary heart disease (n = 94, 26.3%, Table 3).
Table 3: Patients who have the chronic diseases in their medical history.
| One Chronic disease (n =210) | Two Chronic diseases* (n=84) | Three Chronic diseases* (n=26) | ||||||
|---|---|---|---|---|---|---|---|---|
| Chronic Diseases | N | % | Chronic Diseases | N | % | Chronic Diseases | N | % |
| CHF | 30 | 14.3 | CHF | 15 | 17.9 | CHF | 6 | 23.1 |
| CHD | 26 | 12.4 | CHD | 11 | 13.1 | CHD | 6 | 23.1 |
| CA | 23 | 10.9 | CA | 9 | 10.7 | CA | 3 | 11.5 |
| DM | 13 | 6.2 | DM | 5 | 5.9 | DM | 3 | 11.5 |
| HT | 10 | 4.8 | HT | 6 | 7.1 | HT | 2 | 7.7 |
| Other | 108 | 51.4 | Other | 38 | 45.2 | Other | 6 | 23.1 |
CHF: congestive heart failure, CHD: Coronary Heart Disease, CA: cancer, DM: diabetes mellitus, HT: hypertension.
The major complaint of 70.4% (n = 250) of the patients who died was not recorded in the hospital medical database and patient ED chart, because some were unable to verbalize this complaint, as a result of cardiac/respiratory arrest and/or lack of acuity. Among the 115 major complaints that were recorded, the most common was chest pain (n = 43, 40.9%, Table 4).
Table 4: Chief Complaints.
| Complaint | N | % |
|---|---|---|
| Chest Pain | 43 | 40.9 |
| Tightness in Chest | 32 | 30.5 |
| Shortness of Breath | 16 | 15.2 |
| Palpitation | 10 | 9.5 |
| Vomiting | 4 | 3.8 |
| Total | 105 | 100 |
LIMITATIONS
This study was limited because it was a single-center study, which may not make it representative of all patients who die within the ED in Turkey. However, this study provides a general description of deaths that occur in the ED. The retrospective nature of this study means that a definitive diagnosis remains unclear in some causes of death. In addition, three patient files were missing and could not be evaluated.
DISCUSSION
ED admissions and deaths have steadily risen, and deaths account for 0.3% of all patients visiting the ED [3]. In the present study, the mortality rate was even lower at 0.02%. A post-mortem study conducted by coroners on patients who died within the ED found that most deaths were due to acute MI [4]. In another study, Beckett et al. [5] also reported that the majority of deaths in the ED were caused by acute MI. In the present study, 56.6% of deaths were due to acute MI. Shalley et al. [6] found that medical causes accounted for 87% of ED deaths, of which 60% were from cardiac conditions.Further, studies published as long as 30 years ago found that the most common cause of ED death was acute MI or other cardiac conditions.
In our study, the primary cause of death within the ED was cardiovascular disease, in accordance with national statistics [7-10], followed by cerebrovascular disease and respiratory illness. However, although ED deaths result in much anxiety, the frequency of such events is in fact decreasing, by up to 50% [3]; this could possibly assuage any fears held by ED physicians.
Vanbrabant et al. [11] reported that 15.3% of ED deaths are due to trauma. In the present study, the rate of the traumatic deaths was comparatively very low (1.7%). This can be explained either by the fact that people who were exposed to high-energy trauma died at the scene, or by effective rapid hospitalization, with rapid intervention, before patients died within our ED
Although deaths caused by cancer accounted for 15.3% of total ED deaths in Turkey, according to the Health Statistics [7], the mortality rate was 2.8% in our study. In addition, cancer deaths were low in all age groups in our ED.This can be explained by the fact that we did not have an oncology center in our hospital during the study period; our oncology patients were treated in the neighboring provinces.
Vehid et al. [12] reported that most of the ED deaths occurred in patients aged 70 years or above (24.44%), while Isik et al. [13] reported that deaths in patients aged 50 years and over accounted for 75.2% of all ED deaths. In our study, 88.2% of ED deaths occurred in this age group.
With increasing age, patients are referred to EDs with different diseases and the diseases that cause by death vary [14, 15]. Previous studies have shown that deaths caused by respi- ratory and cerebrovascular diseases appear to increase with age [15, 16]. In our study, deaths caused by respiratory system diseases and cerebrovascular diseases occurred at the highest percentage in patients aged 81±114 years.
A total of seven of 10 annual deaths among Americans are from chronic diseases and 133 million of those who die-almost one in every two adults-have at had least one chronic illness [17]. The findings of our study were comparable; 58.8% of patients who died had at least one chronic illness. Multiple chronic diseases are difficult for the emergency physician to diagnose, and these results in treatment delays.
Emergency patients possess characteristics that are different from those of patients seen in the outpatient setting [2, 11, 15]. Karadag et al. [18] found that most common complaints described during one year of ED admissions were chest pain, abdominal pain, general symptoms, nausea or vomiting, and shortness of breath. In our study, the most common major complaint of patients who died within the ED was chest pain. Therefore, all patients presenting in the ED with complaints of chest pain warrant a complete and thorough evaluation.
Baker et al. [2] reported that mortality data for patients attending the ED can be rapidly and easily obtained from an existing hospital information system. However, Vanbrabant et al. [11] found that hospital databases may contain missing data, compared with the actual record. The inadequacy of hospital medical records is a limitation of studies that are conducted in EDs, as information from such death certificates may misrepresent true mortality statistics [19].
Our study showed that only 29.6% of the patients who died had their complaints recorded at the time of admission. A major complaint must be documented, even for patients who present as unconscious, or with respiratory and cardiac arrest, so that improved statistics of deaths in the ED can be maintained for future reference.
CONCLUSION
This study showed that the most common causes of ED death were actually the most common disease processes of the cardiac, respiratory and cerebrovascular systems, and the most frequent diagnosis was acute MI. Traumatic and oncologic causes of death were observed the least frequently. The mortality rate was highest in those patients aged 75 and older, rather than in younger patients. Cardiac diseases were the most prevalent in the patients aged 71-80 years, while diseases of the respiratory and cerebrovascular systems were the most prevalent in the patients aged 81-114 years. The all ED mortality statistics of this present study was in accordance with national statistics. This situation could maybe assuage any fears ED physicians have. Additionally, the recording of the patients' major complaint was mostly incomplete. The records of ED deaths must be meticulously maintained and in greater detail in future, to enable accurate data tracking.
REFERENCES
- Olsen JC, Buenefe ML and Falco WD. (1998). Death in the emergency department. Ann Emerg Med. 31(6):758-65.
- Baker M and Clancy M. (2006). Can mortality rates for patients who die within the emergency department, within 30 days of discharge from the emergency department, or within 30 days of admission from the emergency department be easily measured? Emerg Med J. 23(8): 601-603
- Kanzaria HK, Probst MA and Hsia RY. (2016). Emergency Department Death Rates Dropped By Nearly 50 Percent, 1997-2011. Health Aff (Millwood). 35(7): 1303-1308.
- Kendall IG, Wynn SM and Quinton DN. (1993). A study of patients referred from A&E for coroners post-mortem. Arch Emerg Med. 10(2): 86-90.
- Beckett MW, Longstaff PM, McCabe MJ, Sulch DA, et al. (1987). Deaths in three accident and emergency departments. Arch Emerg Med. 4(4): 227-232.
- Shalley MJ and Cross AB. (1984). Which patients are likely to die in an accident and emergency department? Br Med J (Clin Res Ed). 289(6442): 419-421.
- Turkish Statistical Institute.
- (2013). Disease Burden Final Report, National Burden of Disease and Cost Effectiveness Project. T. C. Ministry of Health Refik Saydam Hifzissihha Central Presidency 2004, Aydogdu Offset Printing. Ankara
- Okyay P, Bilgen MA, Dirlik M and Barut S. (2011). Change in Causes of Death Statistics Between Year 2008-2009 in the Practice and Research Hospital of Adnan Menderes University: An Intervention Study. ADu Tip Fakultesi Dergisi. 12(1): 1-10.
- Korkmaz T and Balaban B. (2014). Consistency Assessment for the Causes of Death as Indicated in the Death Certificates and in ICD Codes. The Medical Bulletin of Haseki Training and Research Hospital. 52: 103-110.
- Vanbrabant P, Dhondt E and Sabbe M. (2004). What do we know about patients dying in the emergency department? Resuscitation. 60(2):163-170.
- Vehid S, Koksal S, Aran SN, Kaypmaz A, et al. (2000). Evaluation of the distribution of deaths occurred at Cerrahpasa Medical School in the year 1998. Cerrahpasa J Med. 31(1): 16-22.
- Isik AF, Demirel B and Senol E. (2004). Are the reported causes of death "Real Death Reason"? T Klin Adli Tip. 1: 111.
- Gulacti U, Lok U, Celik M, Aktas N and Polat H. (2016). The ED use and non-urgent visits of elderly patients.Turk J Emerg Med. 16(4): 141-145.
- Latham LP and Ackroyd-Stolarz S. (2014). Emergency department utilization by older adults: a descriptive study. Can Geriatr J. 17(4): 118-125.
- Lok U, Gulacti U, Ekmekci B, Bulut T, et al. (2017). Predictive and prognostic role of mean platelet volume in patients with first-ever acute ischemic stroke. Neurosciences (Riyadh). 22(2):119-126.
- Kung HC, Hoyert DL, Xu JQ and Murphy SL. (2008). Deaths: final data for 2005. National Vital Statistics Reports. 56(10) 1-16.
- Karadag B, Cat H, Ozturk AO, Basat O, et al. (2010). Patients Admitted to Emergency Outpatient Clinic and Kept Under Observation: A Survey of Three Years. Akad Geriatri. 2: 176-185.
- Quigley M and Burton J. (2003). Evidence for cause of death in patients dying in an accident and emergency department. Emerg Med J. 20(4): 349-351