Previous Issues Volume 1, Issue 1 - 2016
Assessment of Emergency Medicine Resident Accuracy and Effect of a Training Intervention in the Determination of Cervical Size and Effacement Using a Standardized Cervical Training and Examination Model
Dilip Yarabothu1 , Matthew Cauchon2 , James Espinosa3 , Victor Scali4
1Department of Emergency Medicine, Southern New Hampshire Health System, Nashua, NH, USA
2Department of Emergency Medicine, Eastern Connecticut Health Network, Manchester, CT, USA
3Department of Emergency Medicine, Rowan University SOM Kennedy University Hospital, Stratford, NJ, USA
4Program Co-Director, Emergency Medicine Residency, Rowan University SOM
Corresponding Author: James Espinosa, Department of Emergency Medicine, Rowan University SOM Kennedy University Hospital, 18 East Laurel Road, Stratford, NJ 08084, USA, Tel: +1 646 241 5695; E-Mail: [email protected]
Received Date: 24 Feb 2016 Accepted Date: 05 Mar 2016 Published Date: 12 Mar 2016
Copyright © 2016 Espinosa J
Citation: Yarabothu D, Cauchon M, Espinosa J and Scali V. (2016). Assessment of Emergency Medicine Resident Accuracy and Effect of a Training Intervention in the Determination of Cervical Size and Effacement Using a Standardized Cervical Training and Examination Model. Mathews J Emergency Med. 1(1): 001
ABSTRACT
Women who present to the Emergency Department in their second or third trimester complaining of abdominal pain or cramps require an expeditious exam and determination of their status of possible labor. The discernment of cervical size is a core physical finding in assessing the progress of labor. The objectives of this study were to determine the accuracy of emergency medicine residents in determination of cervical dilation and effacement using a standardized cervical training model before and after completion of a training module. The results of this study suggest that a training intervention, using a standardized cervical dilatation and effacement model and associated training module, is associated with a statistically significant improvement in post-test scores in comparison to pre-test scores. It would appear that the training module itself was the prime determinant of this change. Such an increase in accuracy would logically allow an emergency resident to more accurately convey a patient's status, to convey this status to an obstetric physician, and more importantly, make a suitable decision on transferring a patient to definitive care in a safe and timely manner. Future research could involve testing the duration and durability of the training effect.
KEYWORDS
Emergency Medicine Resident Education; Resident Education; Training Determination of Cervical Size; Emergency Department Obstetrical Training; Emergency Delivery Training.
INTRODUCTION
Women who present to the Emergency Department in their second or third trimester complaining of abdominal pain or cramps require an expeditious exam and determination of their status of possible labor. The discernment of cervical size is a core physical finding in assessing the progress of labor[1]. In emergency departments without 24/7 obstetrical coverage, the initial determination of labor, including the assessment of cervical size, is likely to be performed by emergency physicians.Crucial decisions concerning the activity and stage of labor relate to physician assessment of cervical size, as well as effacement.
What is the accuracy of emergency resident physicians in determining cervical size and effacement?
There appears to be little in the emergency medicine literature, other than some general commentary that determination of cervical size and effacement is poorly reproducible among examiners [2].
Anecdotal experience by all of the research team has revealed instances in which there was wide variation between the degree of cervical dilatation and effacement as determined by the initial assessing emergency resident physician in comparison to the determination by the consulting obstetrician. Such variation could have significant consequences.
The first stage of labor is known as the cervical stage. It ends with a fully dilated and fully effaced cervix. This first stage has phases that are crucial to the emergency physician. The first phase, known as the latent phase, is marked by a generally slow process of cervical dilation. It is followed by the active phase, in which more rapid cervical dilation occurs. The active phase begins when the cervix reaches 3 centimeters of dilation. In the third phase (deceleration phase) cervical dilation continues until full dilation.
In multiparous women, the active phase can rapidly progress into the second stage of labor. As noted in Rosen's textbook, (Rosen's Emergency Medicine) most women who deliver in the emergency department arrive in the active phase of the first (cervical) stage or in early stage two of labor. The end of the first cervical stage is marked by a cervical dilation of 10 centimeters [3].
The emergency department is not an optimal location of delivery. The obstetrical suite is better suited in reference to monitoring and delivery equipment, availability of experienced personnel and support for the fetus/newborn.
The goal of this study is to use a standardized cervical dilatation and effacement model to assess the accuracy of emergency residents in reference to cervical dilatation and effacement. The residents will then undergo a training module and will be subsequently retested.
MATERIAL AND METHODS
Objectives of this study
1. To determine the accuracy of emergency medicine residents in determination of cervical dilation and effacement using a standardized cervical training model.
2. To evaluate emergency medicine resident subjects on accuracy of determination of cervical dilatation and effacement after completion of a training module.
Participants: Emergency medicine residents, Rowan/SOM Emergency Medicine Residency Program. The emergency medicine residents in this program range from first year residents (PGY-1, OGME-1) to senior residents (PGY-4, OGME- 4) or combined EM/IM program residents (PGY-5, OGME-5).
Setting: Rowan/SOM Emergency Medicine Residency Program
Design: Prospective, pre and post training module.
A standardized cervical model was used. The cervical model was owned by the Department of Emergency Medicine of UMDNJ-SOM at the time the study took place. [Cervical Gynecology Examination Model, BuyAmag Inc., Carlsbad, CA] Note: None of the research team has any financial or other relationship to the manufacturer of the model. The model had not been previously used in EM training.
The model has six cervical inserts, ranging from 0 dilation/0% effacement to 9 cm dilation/100% effacement. Each examiner examined each of the 6 inserts and provided an estimate of cervical dilation and percent effacement.
Table 1: Cervical training model inserts.
| Dilation | Effacement |
|---|---|
| 0 | 0 |
| 2 | 50 |
| 2 | 100 |
| 5 | 100 |
| 7 | 100 |
| 9 | 100 |
Each participant underwent a training module and was subsequently retested using all 6 inserts.The training module consisted of a period of up to 5 minutes during which the subject examined the inserts (both tactile and visually) in an open-label manner, i.e., with the dilation and effacement clearly marked.The examiner recorded pre-training and posttraining data. In addition, the examiner facilitated the training module.
Repeat training/testing took place until the participants were able to accurately determine 5 of the 6 inserts or a time limit of 20 minutes had been reached, or the subject had completed 7 attempts without accurately determining the inserts. (Testing was terminated with the first endpoint reached) A 5/6 level of accuracy assures that the crucial determination of the shift from the latent phase to the active phase can be determined. This is possible because there are two inserts with 2 cm dilation: one with 50% effacement and one with 100% effacement. The subjects were required to be able to accurately identify at least one of these inserts, either of which is sufficient to accurately anticipate the crucial shift from the latent to the active phase of labor.
The number of attempts needed (testing blocks followed by repeat learning blocks) in order to achieve this level of accuracy were recorded for each participant.
Data was analyzed in reference to pre and immediate posttest performance as well as in reference to the number of attempts needed to achieve the goal of 5 of 6 accuracy minimum for those who require additional training and testing.
The presentation order of the inserts was randomized using a random number generator.
RESULTS
There were 30 participants in the study.The mean pretest score was 20%. [Range=0% to 50%, SEM=.024 (2.4%), SD=0.134 (13.4%)]
The mean post-test score was 85.5%. [Range=33% to 100%, SEM=.031 (3.1%), SD=0.17 (17%)]
The absolute difference between the means of the two groups was 65.5%.
The difference between the pre-test and post-test scores was highly statistically significant. [Student Paired T test, twotailed p=<.0001, z-test for means, p<.0001]
The boxplots and frequency histograms of the pre-test and post-test groups visually display the differences between the distributions of the pre-test and post-test results. (Figure 1, Figure 2). Of the 30 participants, 5 required additional testing. (5/30=16.6%) All 5 (100%) reached the 5/6 correct response endpoint on the first additional testing cycle. The mean test score for this cohort was 93.3% on the retest.[Range=83.3%, SEM=.04 (4%), SD=.09%)The training level of the five was essentially evenly distributed among the first four years of training. There were two PGY-3 residents who required retesting. There were no PGY-5 residents who required retesting.
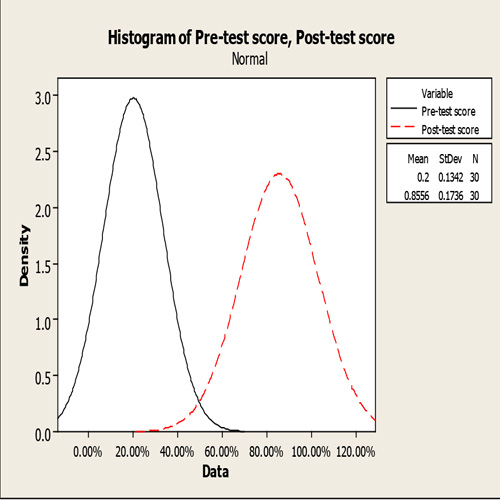
Figure 1: Boxplots, (Box and Whiskers Plot) Pre-test vs Post-test scores
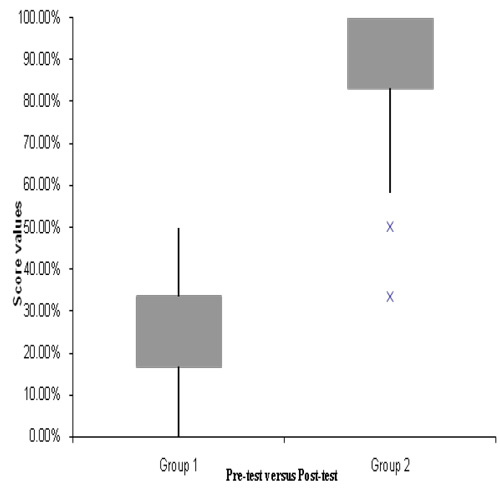
Figure 2:Distribution Histogram, Pre-test vs Post-test scores
The emergency medicine residents have completed their Ob/ Gyn rotation by the end of their third year. The performance of the PGY-1,2,3 group was not statistically different than the performance of the PGY-4,5 cohort, either in the pre-test (p=0.76) or in the post-test (p=0.23).
DISCUSSION
The pre and post intervention results were highly statistically significant. The null hypothesis of no difference in the pretest pretest and post-test group is therefore rejected.
There was no appreciable difference in pre-test or post-test scores as a function of years of training. This suggests no pre-existing tendency was identified in the direction of the development of accuracy as a function of years in training.
Only 17% of the residents required an additional testing cycle. In other words, 83% of the residents demonstrated the predetermined specification of performance based on the initial training module.
There are several limitations to the study. The trainee becomes aware during the training phase that there are a limited number of choices. This is a design issue inherent in using a model. There are more choices, as noted above, around the centrally important sizes related to the crucial determination of the shift from the latent phase to the active phase. The duration and durability of the training effect cannot be determined from this study. The data recorder was not blinded to the insert size. However, the results were objective and numerical in nature (size/effacement) and were not subjective or categorical. Lastly, the study does not prove that outcomes of transfers are improved with increased assessment accuracy.
CONCLUSION
The data suggest that a training intervention, using a standardized cervical dilatation and effacement model and associated training module, is associated with a statistically significant improvement in post-test scores in comparison to pre-test scores. It would appear that the training module itself was the prime determinant of this change.
Such an increase in accuracy would logically allow an emergency resident to more accurately convey a patient's status, to convey this status to an obstetric physician, and more importantly, make a suitable decision on transferring a patient to definitive care in a safe and timely manner.
Future research could involve testing the duration and durability of the training effect.
REFERENCES
- Archie CM. (2007). The Course and Conduct of Normal Labor. In DeCherney et al (Eds) Lange, Current Diagnosis and Treatment, Obstetrics and Gynecology. New York, McGraw Hill.
- Echevaria A and Kuhn G. (2011). Emergencies after 20 weeks of pregnancy and the postpartum period. In Tintinalli et al: Eds: Tintinalli's Emergency Medicine. A Comprehensive Study Guide.New York, McGraw Hill.
- Desai, et al. (2010). Labor and Delivery and Their Consequences. In Marx et al: Eds Rosen's Emergency Medicine. Philadelphia, Mosby Elsevier.