Previous Issues Volume 1, Issue 1 - 2016
HIV-Associated Generalized Papular Mucinosis and Neurosyphilis
Bela Tamasi1,Noemi Mihalik1,Judit Dohan2,Tibor Kovacs3,Judit Harsing1,Bernadett Hidvegi1,Marta Marschalko1,Sarolta Karpati1,Peter Hollo1
1Semmelweis University, Budapest, Hungary, Department of Dermatology, Dermatooncology and Venereology.
2Semmelweis University, Budapest, Hungary, Department of Ophthalmology.
3Semmelweis University, Budapest, Hungary, Department of Neurology.
Corresponding Author: Bela Tamasi, Semmelweis University, Department of Dermatology, Venereology and Dermatooncology, H-1085 Budapest, Hungary.Tel: +361-459-1500; E-Mail: [email protected]
Received Date: 21 Mar 2016
Accepted Date: 30 Mar 2016
Published Date: 01 Apr 2016
Copyright © 2016 Tamasi B
Citation: Tamasi B, Mihalik N, Dohan J, Kovacs T, et al. (2016). HIV-Associated Generalized Papular Mucinosis and Neurosyphilis. Mathews J Dermatol. 1(1): 005.
ABSTRACT
Background and Aims
The association of cutaneous mucinosis with other conditions is frequent. While the rare coexistence of papular mucinosis with HIV infection has already been documented, any relation of the disease to syphilitic infection has not been proved yet. We present on a patient with generalized papular mucinosis, HIV infection and neurosyphilis.
KEYWORDS
Mucinosis; HIV; Syphilis; Neurosyphilis.
INTRODUCTION
Cutaneous mucinoses are characterized by excessive dermal deposition of acid glycosaminoglycans. Dubreuilh was the first to describe lichen myxoedematosus in 1906, and it was in 1953 when Montgomery and Underwood classified the various clinical forms [1]. Association of cutaneous mucinoses with other conditions, such as paraproteinemia, diabetes mellitus, thyroid dysfunction, hepatitis C and HIV-infection, was found frequently [2]. No definite reference about relation to syphilis infection has been published yet. Etiologic factors of dermal mucin deposition have not been clarified, it is assumed that abnormal activation of mucinproducing dermal fibroblasts by autoantibodies, paraproteins and cytokines, or defective pathways of mucin degradation could be involved [3-5]. Here we present an uncommon form of papular mucinosis (PM) associated with HIV infection and neurosyphilis.
CASE REPORT
A 30-year-old, otherwise healthy man presented with widespread skin symptoms of about 12 months duration without any subjective complaints. Widespread 3-5 mm, skin coloured papules suggested scleromyxoedema. Skin biopsy revealed alcian blue and PAS positive mucin deposition in the papillary dermis, perivascular and perifollicular inflammatory infiltrate and discrete epidermal vacuolization. Laboratory examination showed elevated liver enzymes and polyclonal hypergammaglobulinaemia, ANA antibodies were negative. The patient refused the offered thorough examination. After a few months he was hospitalised at an ophthalmologic department because of bilateral visual impairment. Panuveitis was diagnosed on the basis of abnormal perimetry and funduscopy findings. TPPA, TP-ELISA and RPR tests were positive, the latter in 1/512 dilution. Anti-HIV ELISA was reactive. On admission the patient showed widespread indurated, skincoloured papules 2-5 mm in diameter, diffuse alopecia, bilateral inguinal and submandibular lymphadenopathy and he complained of dizziness and headache. No genital symptoms were present (Figure 1).
.jpg)
Figure1: Close-up view of skin symptoms on forearm.
Routine laboratory examination showed increased ESR and serum protein levels with hypergammaglobulinaemia. Examination of the cerebrospinal fluid revealed a cell count of 142/3 and elevated protein levels, CSF-TPPA was positive in 1/160 dilution. MR examination of the brain revealed small subcortical foci in the frontal white matter, macro-vascular abnormality and leptomeningeal contrast enhancement were excluded. HIV infection was verified by Western blot, CD4-count was 258/l, HIV viral load was 61300 copies/ml in the peripherial blood, thus the patient belonged to category A2 according to the CDC Classification System for HIV infection. Repeated skin biopsy showed dermal mucin deposition stained positive with alcian blue with no inflammation or infiltration of plasma cells (Figure 2).
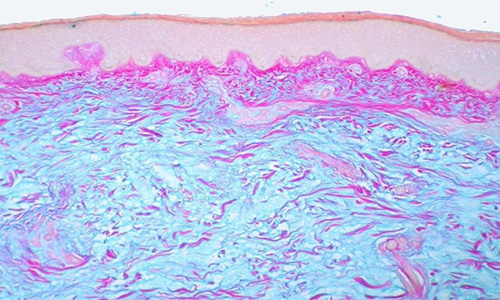
Figure2: Skin biopsy specimen stained with alcian-blue and PAS. Pink stained dermal fibres and blue stained dermal mucin deposition are clearly visible.
Intravenous benzylpenicilline of 6 millions IU q.i.d. for 14 days was administered, preceded by intravenous methylprednisolone supplementation 80 and 40 mg respectively before and on the first day of therapy. As the patients CD4-count was below 300/l, combined antiretroviral treatment with zidovudine, lamivudine, ritonavir and lopinavir has been commenced. On follow-up, the patients skin symptoms have been gradually improving, diffuse alopecia has been resolved.
DISCUSSION
Cutaneous mucinoses are characterized by either localized or generalized deposition of mucin in the skin [2]. The classification of lichen myxoedematosus (LM) dates back to 1953 when Montgomery and Underwood first distinguished four types: (a) discrete papular mucinosis (DPM), (b) scleromyxedema, (c) localized/generalized lichenoid PM and (d) urticarial plaque like PM [2,6]. DPM occurs most frequently and its association with HCV and HIV infections has been observed [7]. Clinically skin-coloured, symmetric papules 2-5 mm in diameter appear on the trunk and proximal parts of extremities with facial sparing. To date 15 cases of PM associated with HIV infection have been described and in 12 cases HIV infection preceded the cutaneous symptoms [7,8]. According to international data, the prevalence of LM among HIV-infected patients is 1:750. The reason why cutaneous mucinoses are associated with HIV infection has not been clarified. The role of direct stimulation of fibroblasts by HIV, elevated cytokine-levels and hyperactive plasma cell function have been studied [5]. There are case reports presenting associated paraproteinemia that may be caused by abnormal cytokine-secretion and B-cell hyperactivation caused by HIV infection [4]. There is no data on syphilisassociated cases of mucinosis to the best of our knowledge [9]. More than 90% of HIV patients present cutaneous symptoms during the course of the infection that may be caused either by virus-mediated destruction of cutaneous Langerhans cells leading to defective immune reactions, or by the global immune-dysfunction of the human host leading to atypical presentation of classic skin diseases [10,11]. These skin conditions, majorly infections, develop during the progression of HIV disease, thus they can show the deteriorating immune status of the infected, or indicate HIV infection if no medical history is available.
CONCLUSION
It is of significance that cutaneous conditions that are known to be associated with HIV infection, like cutaneous mucinosis, draw attention to a possible HIV infection [10]. In the case of papular mucinosis, there is no definite relation to syphilis alone and due to the concomittant treatment in the case of our patient, resolution of skin symptoms cannot be bound exclusively to the use of penicillin or HAART.
REFERENCES
- Rongioletti F. (2006). Lichen myxedematosus (papular mucinosis): new concepts and perspectives for an old disease. Semin Cutan Med Surg 25(2), 100-104.
- Rongioletti F and Rebora A. (2001). Updated classification of papular mucinosis, lichen myxedematosus and scleromyxedema. J Am Acad Dermatol 44(2), 273-81.
- Pandya AG, Sontheimer RD, Cockerell CJ, Takashima A, et al. (1995). Papulonodular mucinosis associated with systemic lupus erythematosus: possible mechanisms of increased glycosaminoglycan accumulation. J Am Acad Dermatol. 32(2), 199-205.
- Depaire-Duclos, Renuy F, Dandurand M and Guillot B. (1998). Papular mucinosis with rapid spontaneous regression in a HIV-infected patient. Eur J Dermatol. 8(5), 353-354.
- Rongioletti F, Ghigliotti G, De Marchi R and Rebora A. (1998).Cutaneous mucinoses and HIV infection. British Journal of Dermatology. 139(6), 1077-1080.
- Bragg J, Soldano CA and Jo-Ann ML. (2008). Papular mucinosis (discrete papular lichen myxedematosus). Dermatology Online Journal. 14(5), 14.
- Concheiro J, Prez-Prez L, Peteiro C, Toribio J, et al. (2009). Discrete papular lichen myxedematosus: a rare subtype of cutaneous mucinosis. Clinical and Experimental Dermatology. 34(8), E608-10.
- Abbott RA, Calonje E, Almaani N, Kulasegram R, et al. (2010). Widespread papules in a patient with human immunodeficiency virus. Clin Exp Dermatol. 35(7), 801-802.
- Dourmishev L and Dourmishev A. (2005). Syphilis: uncommon presentations in adults. Clinics in Dermatology. 23(6), 555-564.
- Tschachler E, Bergstresser PR and Stingi G. (1996). HIVrelated skin diseases. The Lancet. 348(9040), 1511-1512.
- Fodor et al. (2011). HIV-related skin diseases. Borgygyszati s Venerolgiai Szemle. 87, 149-154.