Previous Issues Volume 1, Issue 3 - 2016
Hydranencephaly
Mohammad Nawaz Nasery1, Farhad Farzam1, Hidayatullah Hamidi2, Jamshid Sadiqi2, Ahmad Reshad Faizi2, Fazel Rahman Faizi2, Marzia Mohammadi2
1Radiology department, Ali Abad Teaching Hospital, Kabul, Afghanistan.
2Radiology department, French Medical Institute for Children (FMIC), Kabul, Afghanistan.
Corresponding Author: Mohammad Nawaz Nasery, Ali Abad Teaching Hospital Kabul, Afghanistan, Tel: +93 20 250 0522; E-Mail: [email protected]
Received Date: 28 Jun 2016 Accepted Date: 08 Aug 2016 Published Date: 11 Aug 2016
Copyright © 2016 Nasery MN
Citation: Nasery MN, Farzam F, Hamidi H, Sadiqi J, et al. (2016). Hydranencephaly. Mathews J Case Rep 1(3): 013.
ABSTRACT
Hydranencephaly is an isolated rare congenital brain anomaly in which the greater parts of the cerebral hemispheres are replaced by cerebrospinal fluid (CSF). Bilateral occlusion of the internal carotid arteries mostly in the supraclinoid level in utero is a potential etiology. Clinical features include intact brainstem reflexes without evidence of higher cortical activity. Infants with this condition are normal at birth; however, after a few weeks, they usually become irritable and have increased muscle tone and, after a few months of life, seizures and hydrocephalus (excessive accumulation of CSF in the brain) may develop. Other symptoms are growth retardation, impaired vision, deafness and spastic paralysis. Due to the late onset of most symptoms and signs, the diagnosis may be delayed. The prognosis of hydranencephaly is poor; many of these patients die during their first year. This report presents a case of hydranencephaly diagnosed in an 8-month-old baby.
KEYWORDS
Hydranencephaly; CT scan; CSF; Ventricles; Prenatal; Postnatal; MRI; Ultrasound; Transillumination. Situs Inversus Totalis; Situs Inversus; Dextroacardia.
INTRODUCTION
Hydranencephaly is a rare abnormality of the brain occurring in 1/10,000 births all around the world [1, 2]. It is thought to be arising from vascular insult involving the internal carotid artery after development of brain and ventricles occurs, usually in 2nd trimester of pregnancy; therefore, posterior circulation is intact [1-3]. This results in cortical destruction (most of the cerebral cortex is absent) and forms a large cerebrospinal fluid (CSF) space anteriorly involving the frontal and temporal lobes and intact areas in the posterior circulation, namely preserved thalami [1-4]. The third ventricle is normal, and the falx is seen in the midline [2]. The fetal head circumference would be expected to be normal [2]. Toxoplasmosis and viral infections may cause this abnormality [2]. Toxic exposures and cocaine abuse have been reported, and described in rare syndromes [2]. In monochorionic twin pregnancies, death of one twin in the second trimester may cause a vascular exchange to the living twin through the placental circulation, leading to hydranencephaly in the surviving fetus [2, 7]. This work reports a case of diagnosis of hydranencephaly.
CLINICAL FINDINGS
An eight months female patient was referred for brain computed tomography (CT)-scan to radiology department. She had seizure and gradual enlargement of the head since birth.
IMAGING FINDINGS
CT scan in the patient demonstrated an intact falx with huge fluid density in the supratentorial level associated with separate thalami that suggested the diagnosis of hydranencephaly [Figures 1 and 2]. Presence of the posterior fossa structures but the absence of the cerebral hemispheres confirms that the posterior circulation is of normal limit [Figure 3].

Figure 1: Axial image of brain CT-scan showing an intact falx with huge fluid density in the supratentorial level associated with separate thalami that suggested the diagnosis of hydranencephaly.
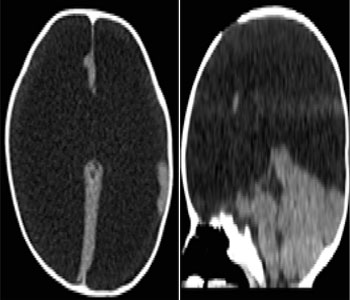
Figures 2A and 2B: Axial (A) and sagittal (B) images demonstrate a complete absence of the cerebral hemispheres, with a small amount of occipital cortex remaining. The absence of a circumferential rim of residual cerebral hemispheric tissue eliminates hydrocephalus as a diagnostic consideration. Posterior fossa structures are intact confirming that posterior circulation is intact.

Figures 3: Axial computed tomography demonstrates an intact falx and large fluid density collection in the supratentorial level with small amount of brain parenchyma adjacent to the falx cerebri.
DISCUSSION
Hydranencephaly is a congenital brain anomaly due to vascular insult and resulting in a CSF filled parenchymal cavity which has not communicate with the subarachnoid space [3]. Posterior fossa structures are preserved because the posterior circulation is intact [2, 3, 4].
CLINICAL PERSPECTIVE
The infant's head size and spontaneous reflexes such as sucking, swallowing, crying, and moving the arms and legs may all seem normal, depending on the severity of the condition. However, after a few weeks, the infant usually becomes irritable and has increased muscle tone (hypertonia) [3]. After several months of life, seizures and hydrocephalus may develop [3]. Diagnosis may be delayed for several months because the infant's early behavior appears to be relatively normal [3].
IMAGING PERSPECTIVE
Diagnosis may be made in utero via standard ultrasound, and confirmed with a high quality ultrasound [3, 5]. Ultrasound, magnetic resonance imaging (MRI) (pre and postnatal) and CT-scan are commonly used to make the diagnosis [5, 6]. Ultrasound examination is a useful diagnostic tool in the prenatal diagnosis of hydranencephaly and shows, at 21 and 23 gestational weeks, which is characterized by the absence of cerebral hemispheres, replaced by an anechoic content filling the supratentorial level. Thalami brain stem, and cerebellum are preserved [5]. After delivery, CT and MRI scan are used to differentiate more accurately hydranencephaly from holoprosencephaly or severe congenital hydrocephalus [5, 6]. In the present case, CT-scan demonstrates replacement of brain parenchyma with fluid density in the supratentorial level. No parenchymal rim remains around the CSF cleft. The residual parenchyma consists of the thalami and posterior fossa which is typical of hydranencephaly. Transillumination is a useful diagnostic tool for diagnosis of hydranencephaly, in absence of other possible neuroradiological examination [5]. According the neurological signs and physical examination of the head in antenatal and postnatal periods, MRI remains the best imaging modality [5]. Electroencephalogram may be useful to confirm the presence and type of seizures, as it relates to their treatment [5]. Angio-MRI is a useful imaging tool to find congenital anomalies of the cerebral vascular structures [5]. The differential diagnosis is severe hydrocephalus, bilateral schizencephaly, and holoprosencephaly [1, 2, 3].
CONCLUSION
Ultrasound is the modality of choice for the diagnosis of hydranencephaly in pre and postnatal period. However, MRI can diagnosis the cases which is poor in ultrasound such as obesity and oligohydramnios with suspected malformation pathology. MRI may confirm the ultrasonography findings, the findings which are not seen in ultrasound and visualizes the fetal anatomy, especially the central nervous system, thorax and abdomen. CT-scan is also used for studying anatomical features if MRI is not available. CT-scan is also used for studying anatomical features if MRI is not available. The case that was reported has typical appearance of hydranencephaly which was diagnosed in postnatal period with CTscan. Essentially, there was no cortical tissue but thalami and posterior fossa were preserved. Often islands of residual tissue are seen typically at the occipital poles and orbitofrontal regions, like in this case. The falx was present and the destroyed brain parenchyma was replaced by CSF.
REFERENCES
- Kurtz AB and Johnson PT. (1999). Case 7: hydranencephaly. Radiolog. 210(2), 419-422.
- Sepulveda W, Cortes-Yepes H, Wong AE, Dezerega V, et al. (2012). J Ultra Med. 31(5), 799-804.
- Pant S, Kaur G and De JK. (2010). Hydranencephaly. KUMJ. 8(29), 83-86.
- Pavone P, Pratic AD, Vitaliti G, Ruggieri M, et al. (2014). Hydranencephaly: cerebral spinal fluid instead of cerebral mantles. Ital J Pediatr. 40, 79.
- Khalid M, Khalid S, Zaheer S, Redhu N, et al. (2012). Hydranencephaly: A rare cause of an enlarging head size in an infant. N Am J Med Sci. 4(10), 520-522.
- Olowu JA, Lagunju IA, Tongo OO and Atalabi M. (2006). Intrauterine fetal death of one of twins, coexisting with hydranencephaly in the surviving co-twin: a case report. West Afr J Med. 25(3), 246-248.