Previous Issues Volume 1, Issue 3 - 2016
Situs Inversus with Dextrocardia
Jamshid Sadiqi1, Mohammad Tahir Aien1, Mohammad Nawaz Nasery1, Hidayatullah Hamidi1
1Department of Radiology, French Medical Institute for Children (FMIC), Kabul, Afghanistan.
Corresponding Author: Jamshid Sadiqi, Department of Radiology, French Medical Institute for Children (FMIC), Kabul, Afghanistan,Tel: 0093747036627; E-Mail:[email protected]
Received Date: 09 May 2016 Accepted Date: 11 Jul 2016 Published Date: 14 Jul 2016
Copyright © 2016 Sadiqi J
Citation: Sadiqi J, Aien MT, Nasery MN and Hamidi H. (2016). Situs Inversus with Dextrocardia. Mathews J Case Rep 1(3): 012.
ABSTRACT
Situs inversus totalis or situs inversus-dextroacardia is a rare congenital anomaly which is characterized by reverse position of adnominal and thoracic viscera. This anomaly was detected in an eight- month-old female baby after a barium enema examination which showed reversed position of colonic frame. The sigmoid and descending colons were located in the right side of abdomen and ascending colon and cecum in the left side. Plain chest x-ray and abdominal ultrasonography confirmed the anomaly by evidence of right side cardiac position and reversed location of abdominal organs, respectively.
KEYWORDS
Situs Inversus Totalis; Situs Inversus; Dextroacardia.
CASE REPORT
An-eight-month- female baby was referred to radiology department of French Medical Institute for Children (FMIC) for barium enema examination due to chronic constipation. During the barium enema examination, reversed position of colonic frame was detected which showed almost normal caliber and haustrations of bowel loops. The sigmoid colon, descending colon and splenic flexure were located in the right side of abdomen while the hepatic flexure and ascending colon were observed in the left side of abdomen (Figure 1).

Figure 1: Abdominal x-ray in anterior posterior supine position shows reversed position of colonic frame.
For evaluation of cardiac position and axis, chest x-ray was preformed which demonstrated right side position of the heart (dextroacardia) with the location of liver in the left side and stomach in the right side of abdomen (Figure 2) also in trans-abdominal ultrasound spleen was seen in the right upper abdomen (Figure 3) and liver in the left upper abdomen (Figure 4) confirming presence of situs inversus dextrocardia.

Figure 2: Chest x- ray demonstrates right side position of heart (dextroacardia) with reversed position of abdominal organs, liver in the left side of abdomen and stomach in the right side of abdomen.
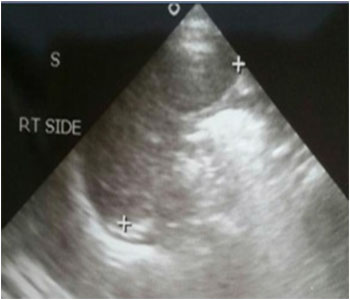
Figure 3: Abdominal ultrasound shows right side position of spleen.
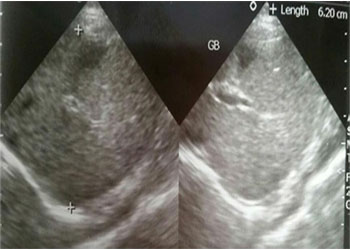
Figure 4: Ultrasound of left upper abdomen demonstrates liver and gall bladder (reversed position).
DISCUSSION
Situs inversus is a term used when internal organs of the body have reversed position or when mirror image of normal internal organ is existed. The total transposition of all thoracic and abdominal viscera is called situs inversus totalis [1]. Dextrocardia is a term used for the reversed position of the heart. This occurs when the heart base to apex orientation is pointed toward the right side of the chest rather than left side (normal position) [2]. Situs inversus dextrocardia is a rare congenital condition which is also called situs inversus totalis. The occurrence of this congenital problem has been variously expressed from 1/6000 to 1/ 35000 of live births [3]. This is an autosomal recessive genetic disorder which the defect occurs in chromosome 14. The primitive loop during embryonic developmental process traverses into the opposite direction of normal position resulting to organ displacement [4]. In situs inversus totalis morphologically left atrium is located in the right side and morphologically right atrium is in the left side, also the lungs have changed their positions, as left lung has three lobes and right lung contains two lobes [2]. Abdominal organs demonstrate reversed position, liver, gall bladder, ligament of Treitz, ileum and ascending colon are in the left side and spleen, stomach, jejunum and descending colon locate in the right side [2]. This congenital anomaly affects both males and females equally. The affected individuals usually have an asymptomatic life but in 3-5% of cases congenital heart diseases can occur. The atrioventricular discordance and transposition of great vessels are the commonest associated abnormalities while the right sided aortic arch occurs in about 80% of cases [5]. Some people with situs inversus suffer from chronic sinusitis, bronchiectasis and nasal polyposis making a syndrome called kartagener syndrome [6]. A very rare type of situs inversus is accompanied with normal left side cardiac position, called situs inversus with levocardia. This anomaly is highly seen with congenital heart diseases which make about 95% of cases. The affected population with Situs inversus dextroacardia usually does not need any specific treatment except when they are symptomatic or whenever any treatable congenital heart anomaly is present. However the recognition of this congenital condition is essential when any interventional procedure or emergency surgery is going to be done in order to avoid any mishaps [7].
CLINICAL PERSPECTIVE
The diagnosis is usually suggested clinically [2]. Signs and symptoms are directly proportional to the level of CO in blood. At lower levels; headache is the commonest symptom, while at higher levels, mental status changes, dyspnea, and syncope may occur. Very high levels of intoxication can result in myocardial ischemia, ventricular arrhythmias, pulmonary edema, lactic acidosis, seizures, hypotension, coma, and death [10]. While the diagnosis is usually made clinically and treatment should be started, imaging is useful for understanding pathophysiologic mechanism, delineation of disease extent and determining the prognosis [1, 2, 11].
REFERENCES
- Benjelloun EB, Zahid FE, Ousadden A and Taleb KA. (2008). A case of gastric cancer associated to situs inversus totalis. Cases journal. 1(1), 391.
- Maldjian PD and Saric M. (2007). Approach to dextrocardia in adults: review. American Journal of Roentgenology. 188(6 Suppl), S39-S49.
- Adeyekun AA, Onunu AN and Mazeli FO. (2004). Dextrocardia with situs inversus: A case report. West African journal of medicine. 22(4), 358-360.
- Demetriades H, Botsios D, Dervenis C, Evagelou J, et al. (1999). Laparoscopic cholecystectomy in two patients with symptomatic cholelithiasis and situs inversus totalis. Digestive surgery. 16(6), 519-521.
- Gutgesell HP. (1997). Cardiac malposition and heterotaxy. Science and practice of pediatric cardiology. 2, 1539-1561.
- Casanova MS, Tuji FM, Yoo HJ and Haiter-Neto F. (2014). Kartagener syndrome. Dentomaxillofacial Radiology. 35(5).
- Radhika, Dabbiru, Saila N, Rekha, et al. (2011). Dextrocardia with situs inversus-a case report. Int J Anat Var. 4, 86.