Previous Issues Volume 1, Issue 3 - 2016
CT Features of Carbon Monoxide Poisoning Induced Brain Ischemic Changes
Hidayatullah Hamidi1, Mohammad Tahir Aien1
1Department of Radiology, French medical institute for children (FMIC), Kabul, Afghanistan.
Corresponding Author: Hidayatullah Hamidi, Department of Radiology, French medical institute for children (FMIC), Kabul, Afghanistan, Tel: 0093 744 733 605; E-Mail:[email protected]
Received Date: 16 Apr 2016 Accepted Date: 05 Jul 2016 Published Date: 07 Jul 2016
Copyright © 2016 Hamidi H
Citation: Hamidi H and Aien MT. (2016). CT Features of Carbon Monoxide Poisoning Induced Brain Ischemic Changes. Mathews J Case Rep 1(3): 011.
ABSTRACT
Carbon monoxide poisoning can cause serious damage to brain and myocardium. The sites more commonly affected in the brain are globus Pallidus, caudate nucleus, putamen, thalamus and cerebral white matter. The authors present a case of Carbon Monoxide poisoning in a 33 year old previously healthy electrician who was exposed unintentionally to generator smoke in a close environment for approximately one hour and the patient was unconscious thereafter. Nonenhanced brain Computed tomography was performed on the third day of exposure and revealed diffuse white matter ischemic changes and brain edema.
IMAGING FINDINGS
Non enhanced axial CT sections were taken through the head with 128 slice Siemens scanner. Diffuse white matter hypodensities were noted in bilateral cerebral hemispheres (Figure 1).

Figure 1: Non enhanced axial CT section: Diffuse white matter hypo-densities are noted in bilateral cerebral hemispheres.
Altered corticomedulary differentiation was also noted with features of brain edema evident by effacement of anterior horns of bilateral lateral ventricles and cortical sulci. (Figure 2)

Figure 2: Non enhanced axial CT section: altered corticomedullary differentiation with effaced anterior horns of bilateral lateral ventricles. The cortical sulci are also effaced due to diffuse brain edema.
Bilateral middle cerebral arteries appeared denser in these non-enhanced CT images, most probably secondary to adjacent parenchymal low attenuation as a result of ischemia and edema. (Figure 3)
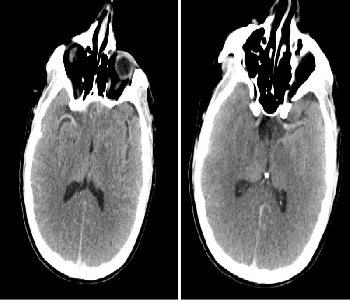
Figure 3: Non enhanced axial CT images: The middle cerebral arteries (MCA) are dense. The right MCA is well seen in right image and the left MCA in left image.
DISCUSSION
BACKGROUND
Carbon monoxide (CO) is a lethal, toxic gas produced by incomplete burning of carbon-based fuels and substances [1]. Intoxication occurs by inhalation of natural gas, smoke or automobile exhaust [2]. CO poisoning can cause serious (acute and delayed) damage to brain and myocardium [3]. Various mechanisms are described responsible for brain damage, the most important being hypoxia [3].
AREAS AFFECTED IN BRAIN
- Globus Pallidus (GP) is the most common site of involvement and the damage occurs immediately [4, 5]. The predilection of GP is unclear but may be due to hypotensive effects of its watershed territory or CO binding to iron-rich GP [5, 6].
- Occasionally caudate nucleus, putamen, and thalamus can also be involved [1].
- Cerebral white matter (WM) is more sensitive than gray matter (GM) to ischemia in early stages [7]. WM demyelination is believed to be responsible for delayed neuropsychiatric syndrome [8].
- Diffuse Hypoxic-Ischemic Encephalopathy can occur, predominantly involving GM. Less frequently focal cortical injury can occur predominantly in temporal lobes and hippocampus [4].
- Brain stem and cerebellar involvement reflect more severe insult because they have a higher resistance to hypoxia [4].
- Neuronal necrosis and apoptotic death can lead to diffuse brain atrophy [9].
CLINICAL PERSPECTIVE
The diagnosis is usually suggested clinically [2]. Signs and symptoms are directly proportional to the level of CO in blood. At lower levels; headache is the commonest symptom, while at higher levels, mental status changes, dyspnea, and syncope may occur. Very high levels of intoxication can result in myocardial ischemia, ventricular arrhythmias, pulmonary edema, lactic acidosis, seizures, hypotension, coma, and death [10]. While the diagnosis is usually made clinically and treatment should be started, imaging is useful for understanding pathophysiologic mechanism, delineation of disease extent and determining the prognosis [1, 2, 11].
IMAGING PERSPECTIVE
CT is usually the first line, rapid imaging modality while MRI can depict the changes more precisely, especially in areas where CT is of limited value; like hippocampus [11]. The main imaging features are those of ischemic insult (hypodensity in CT, low signal on T1WI, high on T2WI and FLAIR images and diffusion restriction) [1].
OUTCOME
Management depends on early diagnosis and initiation of hyperbaric oxygen therapy, as treatment is of benefit in reversing both cerebral and myocardial tissue damage [11]. Based on severity of insult, the prognosis differs from complete recovery, to long-term neurologic sequelae, and even death [2, 10]. Lesions within deep WM are indicator of a poor prognosis and absence of white matter changes at follow up CT suggest likely improvement [2].
REFERENCES
- Chung-Ping L, Shao-Yuan C, Kwo-Whei L, Wei-Liang C, et al. (2007). Brain injury after acute carbon monoxide poisoning: early and late complications. American Journal of Roentgenology. 189(4), W205-W211.
- Miura T, Mitomo M, Kawai R and Harada K. (1985). CT of the brain in acute carbon monoxide intoxication: characteristic features and prognosis. American journal of neuroradiology. 6(5), 739-742.
- Beppu T. (2014). The role of MR imaging in assessment of brain damage from carbon monoxide poisoning: a review of the literature. American Journal of Neuroradiology. 35(4), 625-631.
- O'donnell P, Buxton PJ, Pitkin A and Jarvis LJ. (2000). The magnetic resonance imaging appearances of the brain in acute carbon monoxide poisoning. Clinical radiology. 55(4), 273-280.
- Chu K, Jung KH, Kim HJ, Jeong SW, et al. (2004). Diffusionweighted MRI and 99mTc-HMPAO SPECT in delayed relapsing type of carbon monoxide poisoning: evidence of delayed cytotoxic edema. European neurology. 51(2), 98-103.
- Kinoshita T, Sugihara S, Matsusue E, Fujii S, et al. (2005). Pallidoreticular damage in acute carbon monoxide poisoning: diffusion-weighted MR imaging findings. American Journal of Neuroradiology. 26(7), 1845-1848.
- Sener RN. (2003). A cute carbon monoxide poisoning: diffusion MR imaging findings. American journal of neuroradiology. 24(7), 1475-1477.
- Chang KH, Han MH, Kim HS, Wie BA, et al. (1992). Delayed encephalopathy after acute carbon monoxide intoxication: MR imaging features and distribution of cerebral white matter lesions. Radiology. 184(1), 117-122.
- Omaye ST. (2002). Metabolic modulation of carbon monoxide toxicity. Toxicology. 180(2), 139-150.
- Davin KQ, McGahee SM, Politte LC, Duncan GN, et al. (2009). Complications of carbon monoxide poisoning: a case discussion and review of the literature. Prim Care Companion J Clin Psychiatry. 11(2), 74-79.
- Silver DAT, Cross M, Fox B and Paxton RM. (1996). Computed tomography of the brain in acute carbon monoxide poisoning. Clinical radiology. 51(7), 480-483.