Previous Issues Volume 2, Issue 2 - 2017
Percutaneous Closure of Adult Atrial Septal Defects in Adults: Short- and MediumTerm Results
Nejeh Ben Halima1 , Yosra Messaoudi1 , Ahmed Sghaier1 *, Houssem Thabet1, Afef Lagren1, Essia Boughzela2
1Cardiology department of IBN EL JAZZAR university hospital – Kairouan. 2Cardiology department of Sahloul university hospital – Sousse.
Corresponding Author: Ahmed Sghaier, Cardiology department of IBN EL JAZZAR university hospital – Kairouan, Tel: 0021621231994; E-Mail: [email protected]
Received Date: 12 Sep 2017 Accepted Date: 19 Sep 2017 Published Date: 21 Sep 2017
Copyright © 2017 Sghaier A
Citation: Sghaier A, Halima NB, Messaoudi Y, Thabet H. (2017). Percutaneous Closure of Adult Atrial Septal Defects in Adults: Short- and Medium-Term Results. Mathews J Cardiol. 2(2): 015.
ABSTRACT
Introduction: Atrial septal defect (ASD) is the third most common form of congenital heart defects. Controversy still exists regarding its closure in patients > 40 years-old. Few data exist on symptomatic relief and echographic parameters improvement gained after ASD closure in patients over 40 years of age.
Aim: Analyze the efficacy and safety of the percutaneous closure technique in a community of adults aged over 40 years-old with (ASD) eligible for percutaneous closure.
Methods: This is a retrospective study that included patients aged over 40 years-old who had percutaneous ASD closure between 2005 and 2013 at the cardiology department of Sahloul university hospital. Follow-up at 24 hours, 7days, 6 months, and yearly included physical examination, electrocardiogram and transthoracic echocardiography; furthermore, telephone interviews were conducted to determine clinical symptomatic status.
Results: There were 27 patients with a mean age of 47 years (from 40 to 65); 7 were aged more than 60 years-old. There were 23 women. 24 patients had clinically significant symptoms due to their ASDs, including dyspnea (22), palpitations (10), fatigue (6), chest pain (10), and dizziness (2). 3 patients reported no symptoms prior to ASD closure. The mean size of ASD as measured by transesophageal echocardiography was 26,443mm ±6, 8 (from 12 mm to 38 mm). The mean pulmonary artery pressure (PAP) was 42, 95 mmHg ± 8, 04. The mean right ventricle diameter was 40, 6 mm ± 3,3 (35mm, maximum = 45mm). A total of 26 patients had successful defect closure, in one patient, this could not be done due to unusual anatomy of left atrium. The Amplatzer device was used in 25 patients. The mean device size used for all patients was 27, 82 ± 6, 63 mm. There were no major complications. Symptomatic improvement was observed: 20 patients became asymptomatic. At 1year post procedure, the right ventricle diameter showed a statistically significant decrease 34 - + 6 mm (P < 0,001).
Conclusion:This study provided further evidence that transcatheter device closure of ASDs in adults over the age of 40 years is safe, effective, and results in symptomatic relief and regression of pulmonary pression and right ventricle size. Thus, we suggest that percutaneous closure of ASDs in adult patients greater than 40 years of age should be the first option of management.
KEYWORDS
Atrial Septal Defect; Percutaneous Closure; Adults; Congenital Heart Disease.
INTRODUCTION
Atrial septal defect (ASD) is the most common congenital heart disease in adults (30%) [1]. It is responsible for significant morbidity and decreased life expectancy [2, 3]. Percutaneous closure is a reliable alternative to surgery even if it generates some discomfort and significant morbidity. Although this technique has become a standard procedure in most children and young adults, data on success rates and mediumterm outcomes for adults are limited. The aim of this study is to analyze the efficacy and safety of the percutaneous closure technique in a community of adults aged over 40 years-old with ASD eligible for percutaneous closure.
POPULATION AND METHODS
Study TypeThis is a retrospective study that included patients aged over 40 years-old who had percutaneous ASD closure between 2005 and 2013 at the cardiology department of Sahloul university hospital.
Population Patients aged 40 years and older with an ASD with a percutaneous closure indication. Indications for closure were: an important left to right shunt (signs of right ventricular overload) regardless of the presence of symptoms, patients with severe pulmonary vascular disease (pulmonary resistances) 5 units Wood), after a vaso-reactivity test or after a targeted treatment. Were not considered for the percutaneous closure, patients with a septal defect diameter exceeding 38 mm (on transesophageal echocardiography (TEE)) or after using a calibration balloon) and those with inadequate morphology (insufficient shorelines, Multiple defects, complex aneurysm, association of other important lesions).
Echocardiography Complete transthoracic echocardiography (TTE), including M mode, 2D, continuous, pulsed colour Doppler were performed prior to surgery and on each follow-up visit. TEE was routinely performed in all patients proposed for percutaneous closure in order to evaluate the ASD morphology and exclude additional lesions, such as pulmonary venous return abnormality. The right ventricle size was studied by measuring its diastolic diameter on the parasternal long axis view (RVTDD), and systolic pulmonary arterial pressure (SPAP) was estimated from the tricuspid regurgitation rate [4]. The ratio of flow rates (Qp/ Qs) was obtained by measuring the time-velocity, as well as the diameters of the pulmonary artery and the left ventricular ejection pathway [5].
The hemodynamic study An invasive assessment was performed before surgery when the SPAP estimated in ultrasound was greater than 50% of the systemic pressure or 60 mmHg. In these patients, pulmonary vascular resistance (PVR) had been carefully evaluated. Only patients with PVR = 5 units Wood -either spontaneously or after a vaso-reactivity test with nitrogen monoxide-were considered for the ASD percutaneous closure. In patients with left atrial pressure greater than 15 mmHg during invasive assessment, ASD balloon occlusion was performed and pressure measurement was repeated. In patients with an increased left atrial pressure of more than 10 mm Hg, treatment of heart failure was initiated prior to ASD closure to reduce after surgery left heart failure risk.
Interventional catheterization All procedures were performed under general anaesthesia with endotracheal intubation; and guided by x-ray and TEE. Anti-platelet aggregation therapy based on aspirin (100 mg / day) was started at least 2 days before and maintained for at least 6 months after surgery. A dose of intravenous heparin was administered during the procedure.
Follow-up Patients underwent a series of follow-up examinations at 1 day, 1 week, 3-6 months, 12 months, and then every year. Including clinical examination, electrocardiogram and TTE. Particular attention has been paid to determining the functional status and obtaining information on the onset of symptoms or complications.
STATISTICAL ANALYSIS
The data was entered and analyzed using the SPSS 18.0 software. The correlations between the different parameters were tested by simple linear correlation of Bravais Pearson. Their threshold of significance is then tested by the Student test. The alfa risk is set for all tests at 5%.
RESULTS
General characteristics of the population There were 27 patients, 23 women and 4 men. The mean age was 47 years-old with extremes between 40 and 65 years. There were 7 patients aged 60 years or older. Hypertension was found in 6 patients. Diabetes mellitus in 2 patients. The rest did not have any particular pathological history. 21 cases had a sinus rhythm, others were on permanent atrial fibrillation.
Reported symptoms The ASD diagnosis was a fortuitous finding in 3 patients who were totally asymptomatic. Shortness of breath and limitation of functional ability to exercise were the most frequently reported symptoms. 10 patients reported palpitations (Table 1). Of the patients with dyspnea, 17 were NYHA class II, 4 were class III and 1 were class IV. The percentage of symptomatic patients with dyspnea in group A (age < 60 years was 75%). All patients > 60 years-old (100%) were symptomatic of dyspnea and 3 (50%) complained of palpitations.
Reported symptoms ASD anatomy and its consequences on the right cavities: The majority of ASD were central ostium secundum (Figure 1). Of the patients with dyspnea, 17 were NYHA class II, 4 were class III and 1 were class IV. The percentage of symptomatic patients with dyspnea in group A (age < 60 years was 75%). All patients > 60 years-old (100%) were symptomatic of dyspnea and 3 (50%) complained of palpitations
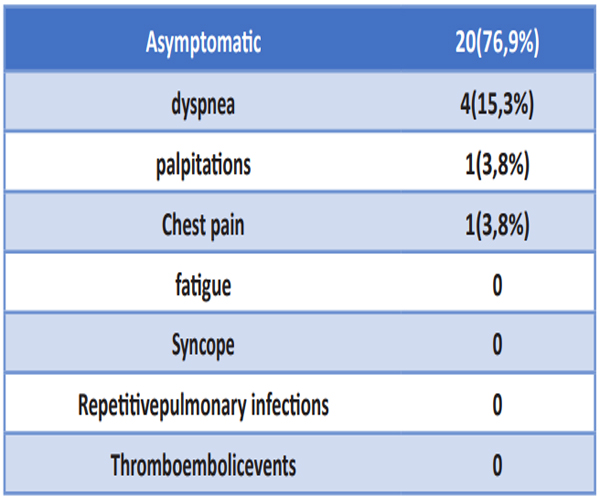
Table 1: Symptoms at diagnosis.
ASD anatomy and its consequences on the right cavities:
The majority of ASD were central ostium secundum (Figure 1).

Figure 1: ASD anatomy on echography.
Aortic edges were absent in 9 cases (33.3%). The mean ASD diameter in TTE was estimated at 25.8 mm with extremes ranging from 10 to 36 mm. In TEE, the mean diameter was 26.43 ± 6.8mm: the smallest ASD measured 12 mm in diameter and the largest 38 mm. The balloon calibration technique was not used in all patients (only 8 patients: minimum diameter = 22 mm, maximum diameter = 38 mm). There was a dilation of the right cavities in all cases. The diastolic diameter of the right ventricle RVTDD was 40.6 mm ± 3.3 (minimum = 35 mm, maximum = 45 mm). The SPAP was at 42.95 mmHg ± 8.04 [28 mmHg up to 60 mmHg]. Overall, there was an increase in SPAP with age, although some elderly patients had a normal SPAP. A correlation was found, but not statistically significant, between the SPAP value and the ASD closure age (R2 = 0.042, p = 0.3). On the other hand, there was a positive and statistically significant correlation between the ASD diameter measured at the TEE and the value of the SPAP, as well as the RVTDD (Figure 2).
Pulmonary arterial pressure was linked to the functional class with a SPAP of 33 ± 9, 42 ± 12 and 50 ± 15 mm Hg for respectively NYHA Class I, II, and III patients (P < 0.0001). The SPAP obtained by echocardiography was on average 10 mm Hg higher than that measured by catheterization during the general anaesthesia.
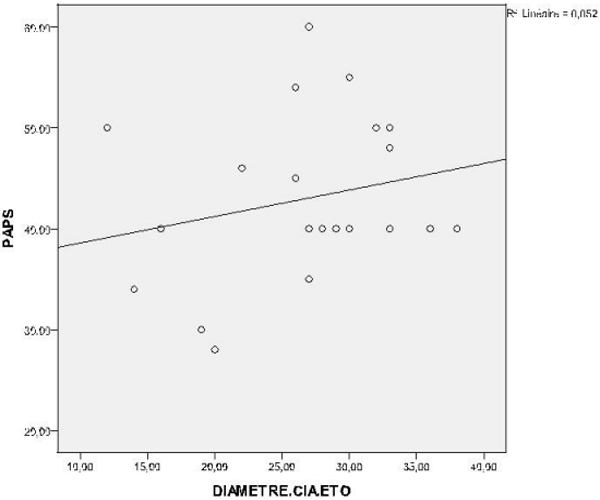
Figure 2: SPAP according to ASD diameter.
Interventional catheterization and per-procedural complications The ASD percutaneous closure was performed with 2 types of prostheses: Amplatzer for 25 patients and a Figulla for 2 cases with a size of 24 and 34 mm respectively. The average diameter of the Amplatzer prosthesis was 27.82 ± 6.63 mm (12 to 38m). The mean time of the procedure was 40 min (30 to 55 min), and the fluoroscopy mean duration was 10.3 min (5.6 o 12.8 min). No procedure-related death was observed. No major complications occurred during the procedure. Paroxysmal passages of supraventricular arrhythmias spontaneously resolved during the procedure were observed in 19 patients among the 21 in sinus rhythm. A single hematoma was observed in 2 patients. At the end of the procedure, 2 patients had new passages of supraventricular rhythm disorders: 1 case of atrial fibrillation and 1 case of junctional tachycardia of spontaneous resolution. One patient developed sinus bradycardia at 40 c / min with good spontaneous evolution. There was only 1 case of procedural failure due to a particular anatomy of the left atrium.
Early complications and residual shunts (First day to 3 months follow-up) 3 patients developed a small pericardial effusion, which disappeared spontaneously within 3 months. One patient developed gastrointestinal haemorrhage secondary to the oral anticoagulant treatment given for atrial fibrillation. No moderate or severe residual shunt was observed. Although a minimal residual shunt was frequently observed on the first day after the procedure, no patients had residual shunt after 3 months of follow-up. No case of atrial fibrillation occurred during the follow-up. (Except one case occurring immediately after the procedure).
Medium-term outcomes (beyond 6 months of follow-up) A clear improvement in symptoms was observed in all age groups (Table 2)
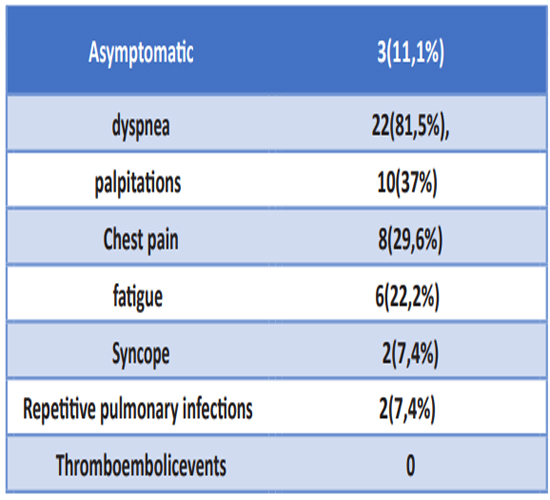
Table 2: symptoms 6 months after ASD percutaneous closure.
Five patients with persistent atrial fibrillation experienced persistent arrhythmias. However, 2 patients with persistent atrial fibrillation experienced a return to sinus rhythm during follow-up. Follow-up by Holter revealed the appearance of frequent atrial extra systoles in a patient who was in sinus rhythm before the procedure. A decrease in RV size and SPAP was observed in all age groups. The RVTDD decreased from 40.6 ± 3.3 mm at baseline to 38 ± 6 mm (P < 0.0001) on the first post-procedural day to 36 ± 6 mm after 1 month and 34 ± 6 mm after 1 year of follow-up. SPAP decreased from 42 ± 5 mmHg per procedural to 35 ± 13 mmHg on the first day and 34 ± 12 mm Hg at 3 months after ASD closure (P < 0.0001) remaining stable (33 ± 14 mmHg) at the end of the follow-up (Figure 3). Absolute variations did not differ significantly between groups (decrease in RV size of 8 ± 7 for patients under 60 years old (group A) and 8 ± 6 mm for patients up to 60 years old (group B), P = 0.80); decrease of SPAP by 8 ± 9 and 9 ± 14 respectively, p = 0.24). Therefore, elderly patients with significantly larger RV and higher SPAP prior to ASD closure ended with a larger RV and a higher SPAP after the procedure.
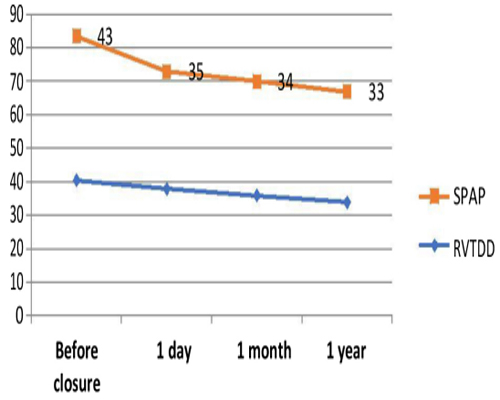
Figure 3: Evolution of SPAP and RVTDD after ASD.
DISCUSSION
The advantage of ASD closure in adults, especially those of advanced age, remains a subject of debate [6-8]. There are very little data from controlled studies on the treatment of ASD.
ASD percutaneous closure safety of ASD percutaneous closure in elderly patients has the advantage of being much less invasive and associated with shorter hospitalization duration than surgery [9, 10]. In the currently published series, including this work, no case of procedure related death was observed. In contrast, ASD surgical closure was associated with a significant increase in mortality in elderly patients [11,12] despite the fact that those sent for surgery were low-risk patients. A study [13] compared the two techniques showed no death in the surgical group (n = 533) and intervention group (n = 751), but a higher rate of serious in-hospital complications in the surgery group (16% versus 3.6% in the intervention group, p = 0.002). The most fatal early complication is the occurrence of a tamponade due to erosion by the prosthesis. Its frequency is estimated to be about 0.1% [14]. It usually occurs within a week of implantation and requires urgent evacuation.
BENEFITS OF ASD PERCUTANEOUS CLOSURE ON THE DIFFERENT PARAMETERS STUDIED
Arrhythmias The incidence of atrial fibrillation, one of the leading causes of morbidity in patients with ASD is closely related to age [15]. An increased risk of occurrence of atrial fibrillation, compared to the general population, is observed in follow-up of patients aged 40 years or older who had surgical or interventional correction of their ASD [15-18]. The surgical series with a followup = 20 year show a low incidence of arrhythmias when the correction is performed before the age of 25 years-old [17, 19]. The effect of percutaneous closure on the risk of late arrhythmias remains a subject of debate, as we do not yet have large cohorts and follow-up sufficiently long to judge. It is likely that the results of the percutaneous closure will also be good, especially since the risk of scar flutter after atriotomy no longer exists and that the percutaneous closure is accompanied by a lesser disturbance of the chronotropic response. Nevertheless, transient atrial fibrillation can be triggered very early after ASD percutaneous closure [20]. Also, the role played by CEC caused atrial ischemia is not found in the percutaneous closure which can help reduce the risk of atrial arrhythmias after this treatment. In our study, 7.4% of patients developed atrial fibrillation within 3 months after the procedure. The sinus rhythm was restored in all cases emphasizing its transient nature potentially caused by the mechanical irritation of the interatrial septum. Silversides et al. [21] reported a greater likelihood of permanent sinus rhythm after ASD percutaneous closure in patients less than 40 years of age and without previous history of arrhythmia. A preventive effect of ASD closure on the long-term incidence of atrial arrhythmias has been described [22]. While persistent atrial fibrillation is less likely to be affected by percutaneous closure, paroxysmal fibrillation may improve after the procedure and its probability may even decrease with age [15]. In summary, atrial arrhythmia is the primary morbidity observed early after percutaneous closure, mainly in elderly patients. The delayed rhythmic risk due to atrial remodelling depends on the precocity of the interatrial shunt correction. This implies regular cardio logical monitoring for patients who have had a late closure (in the absence of residual echocardiographic shunt), in order to manage a thromboembolic risk in time and correctly. The therapeutic attitude towards these patients remains empirical because there are no controlled studies and in this context oral anticoagulation can be proposed for 3 months with a relay by an antiplatelet agent for another 3 months because of the risk of early arrhythmias. A combination of two antiplatelet agents (75mg / day aspirin and 75mg / day clopidogrel) is sometimes used instead of the oral anticoagulant
Functional status Controversial data have been reported concerning the effect of late ASD surgical closure on functional status improvement [23]. The majority of symptomatic patients prior to closure reported functional improvement. Patients classified as asymptomatic have shown an increase in their maximum oxygen uptake to 6 months [24]. Our study was based on symptomatic patients before the ASD closure. However, we found that some patients thought to be asymptomatic reported subjective improvement in various parameters (dyspnea, asthenia and palpitations) after the procedure. Moreover, the majority of patients improved their quality of life.
Pulmonary arterial hypertension The prevalence of pulmonary arterial hypertension in patients with ASD is estimated to be between 6 and 27% [25, 26]. Yong et al [27] reported that patients with advanced PAH have significantly lower PAP but never reaching normal values. PAP decreases at least partially after ASD closure, due to decreased pulmonary flow and probably also due to decreased pulmonary vascular resistance (PVR). Although we cannot provide hemodynamic monitoring data, it is likely that persistent elevation of PVR is the reason for the persistence of a high SPAP in some of our patients. There was a close relationship between PAP and functional status
Right ventricular remodelling Closure of the atrial septal defect results in a significant reduction in RV size and an increase in left ventricular volume [28, 29]. Reduction in RV size occurs immediately after ASD closure and is maintained within the next 3 to 6 months [30]. This study shows that a significant reduction in the RV size can be observed even in elderly patients, although the latter have the largest ventricular volumes before and after the procedure.
Mortality Nowadays the ASD percutaneous closure can be carried out with a mortality almost close to zero, even in the elderly group. An overall benefit of the mortality intervention is even more likely. However; it would never be proven in a randomized trial because it would be unethical to conduct such a study today.
REFERENCES
- Hoffman JIE and Kaplan S. (2002). The incidence of congenital heart disease. J Am Coll Cardiol. 39(12): 1890-1900
- Baumgartner H, Bonhoeffer P, De Groot NM, deHaan F, et al. (2010). ESC Guidelines for the management of grownup congenital heart disease. Eur Heart J. 31(23): 2915- 2957.
- Lindsey JB and Hillis LD. (2007). Clinical update: atrial septal defect in adults. Lancet. 369(9569): 1244-1246.
- Lang RM, Bierig M, Devereux RB, Flachskampf FA, et al. (2005). Recommendations for chamber quantification. J Am Soc Echocardiogr. 18(12): 1440-1463.
- . Dittmann H, Jacksch R, Voelker W, Karsch KR, et al. (1988). Accuracy of Doppler echocardiography in quantification of left to right shunts in adult patients with atrial septal defect. J Am Coll Cardiol. 11(2): 338-342.
- Konstantinides S, Geibel A, Olschewski M, Lothar Görnandt, et al. (1995). A comparison of surgical and medical therapy for atrial septal defect in adults. N Engl J Med. 333: 469-473.
- Du ZD, Hijazi ZM, Kleinman CS, Silverman NH, et al. (2002). Comparison between transcatheter and surgical closure of secundum atrial septal defect in children and adults. J Am Coll Cardiol. 39(11): 1836-1844.
- Lindsey JB and Hillis LD. (2007). Clinical update: atrial septal defect in adults. Lancet. 369(9569): 1244-1246.
- Butera G, Romagnoli E, Carminati M, Chessa M, et al. (2008). Treatment of isolated secundum atrial septal defects: impact of age and defect morphology in 1,013 consecutive patients. Am Heart J. 156(4): 706-712.
- Majunke N, Bialkowski J, Wilson N, Szkutnik M, et al. (2009). Closure of atrial septal defect with the Amplatzer septal occluder in adults. Am J Cardiol. 103(4): 550-504.
- Humenberger M, Rosenhek, Gabriel H, Rader F, et al. (2011). Benefit of atrial septal defect closure in adults: impact of age. Eur Heart J. 32(5): 553-560.
- Gatzoulis MA, Redington AN, Somerville JS and Shore DF. (1996). should atrial septal defects be closed in adults. Ann ThoracSurg. 61(2): 657-659.
- Butera G, Carminati M, Chessa M, Youssef R, et al. (2006). Percutaneous versus surgicalclosure of secundum atrial septal defect: comparison of early results and complications. Am Heart J. 151(1): 228-234.
- Amin Z, Hijazi ZM, Bass JL, Cheatham JP, et al. (2004). Erosion of Amplatzer septal occluder device after closure of secundum atrial septal defects: review of registry of complications and recommendations to minimize future risk. Catheter Cardiovasc Interv. 63(4): 496-502.
- Spies C, Khandelwal A, Timmermanns I and SchräderR. (2008). Incidence of atrial fibrillation following transcatheterclosure of atrial septal defects in adults. Am J Cardiol. 102(7): 902-906.
- Attie F, Rosas M, Granados N, Zabal C, et al. (2001). Surgical treatment for secundum atrial septal defects in patients > 40 years old. J Am Coll Cardiol. 38(7): 2035-2042.
- Murphy JG, Gersh BJ, McGoon MD, Mair DD, et al. (1990). Long–term outcome after surgical repair of isolated atrial septal defect. Follow-up at 27 to 32 years. N Engl J Med. 323(24): 1645-1650.
- Vecht JA, Saso S, Rao C, Dimopoulos K, et al. (2010). Atrial septal defect closureis associated with a reduced prevalence of atrialtachyarrhythmia in the short to medium term: a systematic review and meta-analysis. Heart. 96(22): 1789-1797.
- . Roos-Hesselink JW, Meijboom FJ, Spitaels SE, van Rijen EH, et al. (2003). Excellent survival and low incidence of arrhythmias, stroke and heart failure long-term after surgical ASD closure at young age. A prospective follow-up study of 21-33years. Eur Heart J. 24(2): 190-197
- Chessa M, Carminati M, Butera G, Bini RM, et al. (2002). Early and late complications associated with transcatheter occlusion of secundum atrial septal defect. J Am Coll Cardiol. 39(6): 1061-1065
- Silversides CK, Haberer K, Siu SC, Webb GD, et al. (2008). Predictors of atrial arrhythmias after device closure of secundum type atrial septal defects in adults. Am J Cardiol. 101(5): 683-687.
- Giardini A, Donti A, Sciarra F, Bronzetti G, et al. (2009). Long-term incidence of atrial fibrillation and flutter after transcatheter atrial septal defect closure in adults. Int J Cardiol. 134(1): 47-51.
- Shah D, Azhar M, Oakley CM, Cleland JG, et al. (1994). Natural history ofsecundum atrial septal defect in adults after medical or surgical treatment: a his- torical prospective study. Br Heart J. 71 (3): 224-227, discussion 228.
- Brochu MC, Baril JF, Dore A, Juneau M, et al. (2002). Improvement in exercise capacity inasymptomatic and mildly symptomatic adults afteratrial septal defect percutaneous closure. Circulation 106(14): 1821-1826.
- Balint OH, Samman A, Haberer K, Tobe L, et al. (2008). Outcomes in patients with pulmonary hypertension undergoing percutaneous atrial septal defect closure. Heart. 94(9): 1189-1193.
- . Sachweh JS, Daebritz SH, Hermanns B, Fausten B, et al. (2006). Hypertensive pulmonary vascular disease in adults with secundum or sinus venosus atrial septal defect. Ann ThoracSurg. 81(1): 207-213.
- Yong G, Khairy P, De Guise P, Dore A, et al. (2009). Pulmonary arterial hypertension in patients with transcatheter closure of secundum atrial septal defects: a longitudinal study. Circ CardiovascInterv. 2(5): 455-462.
- Schussler JM, Anwar A, Phillips SD, Roberts BJ, et al. (2005). Effect on right ventricular volume of percutaneous Amplatzer closure of atrial septal defect in adults. Am J Cardiol. 95(8): 993-995.
- Teo KS, Dundon BK, Molaee P, Williams KF, et al. (2008). Percutaneous closure of atrial septal defects leads to normalisation of atrial and ventricular 30.volumes. J Cardiovasc MagnReson. 10: 55.
- Sun P, Wang ZB, Xu CJ, Yang SM. et al. (2008).Echocardiographic and morphological evaluation of the right heart after closure of atrial septal defects. Cardiol Young. 18(6): 593-598.